Mammographic Finding in DCIS
The most common mammographic finding in DCIS is the presence of heterogeneous or fine pleomorphic calcifications with linear-branching pattern.
DCIS also may manifest as a mass or architectural distortion.
A low-grade lesion without necrosis is less likely to manifest with calcifications than either an intermediate or a high-grade lesion.
The extent of DCIS involvement is frequently underestimated at mammography.
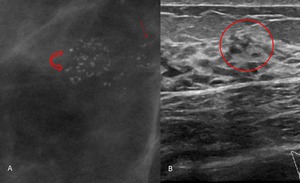
Fig. 1: 52-year-old asymptomatic woman.
A- Magnified view from a follow-up mediolateral mammogram shows fine linear-branching calcifications (straight arrow) as well as amorphous and fine pleomorphic calcifications (curved arrow) in the upper outer quadrant. B- US image demonstrates calcifications within ducts.
Stereotactic biopsy revealed high-grade DCIS
Ultrasound (US) Findings
The US features of DCIS can be subtle and nonspecific.
When calcifications are identified at mammography,
US can be performed to evaluate for an invasive component and to allow possible US-guided biopsy.
Increased breast density may obscure an underlying invasive component at mammography,
and US may show that disease is more extensive than the calcifications evident at mammography.
In addition,
in the setting of extensive high-nuclear-grade DCIS,
in which histologic sampling is more likely to miss microscopic foci of invasive disease,
US can be used to assess the axillary lymph nodes for evidence of invasion.
Calcified DCIS
Calcified DCIS most commonly manifests as echogenic foci located within a mass or duct,
associated with internal microlobulations,
or distributed in a branch pattern.
US resolution for calcifications,
on the order of 200–500 μm,
is less than the 50–100-μm resolution of mammography.
Malignant calcifications are more frequently visualized at US than are those associated with benign tissue,
in which they may be obscured by echogenic breast parenchyma.
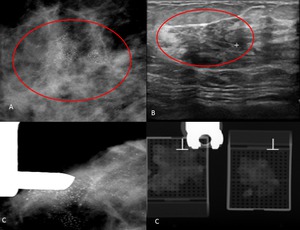
Fig. 2: 59-year-old asymptomatic woman.. A- Lateral spot magnification mammogram demonstrates segmental pleo¬morphic calcifications in the right breast. B- US image demonstrates a hypoechoic mass with lobulated and angular margins and calcifications. C- Stereotactic biopsy revealed high-grade DCIS.
The presence of an associated mass increases the conspicuity of calcifications and confers a greater likelihood of invasive cancer compared with calcifications seen at mammography alone.
Microcalcifications with associated ductal changes are the most common US finding of high-grade DCIS.
Less frequently,
calcifications may appear as echogenic regions without significant mass or duct changes.
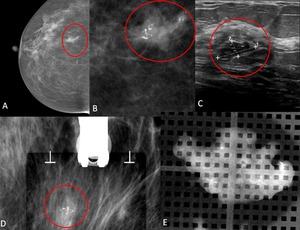
Fig. 3: 47-year-old woman with a palpable mass in the right breast. A- Right Craniocaudal Mammograms B- Lateral spot magnification mammogram demonstrates segmental pleo¬morphic calcifications corresponding to the palpable abnormality.
C- US image demonstrates a hypoechoic mass with microlobulated and angular margins and calcifications. D,E- Stereotactic biopsy revealed high-grade DCIS.
Non calcified DCIS
DCIS may manifest as a mass or asymmetry at mammography.
Masses are more frequently found in non-high-grade than high-grade DCIS.
Non calcified DCIS,
which is more often identified in symptomatic patients,
may manifest as an irregular hypoechoic mass,
but they can also be oval or round,
with microlobulated margins and no posterior acoustic features,
or it may have a “pseudomicrocystic” appearance.
Ductal extension,
seen as a projection extending radially from the mass into a duct,
may be present and represents ductal spread of cancer cells.
When noncalcified DCIS manifests as a cluster of cysts or a complex cystic mass,
there may be associated internal vascularity,
often oriented perpendicular rather than parallel to the wall of the mass.
This is in contrast to clusters of cysts,
which are typically avascular at color Doppler.
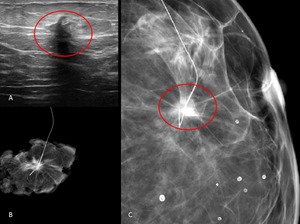
Fig. 4: 49-year-old woman with a palpable mass in the left breast. A- US image demonstrates a hypoechoic nodule. B- spot magnification mammogram after tumorectomy surgery.
C- Right Craniocaudal Mammograms with nodular densification of non calcified DCIS taken just after harpoon colocation.
Manifestations of DCIS at Breast MR Imaging
Magnetic resonance (MR) imaging is commonly performed in the preoperative setting for breast cancer to identify the extent of disease,
and to assess for both ipsilateral foci of multifocal or multicentric involvement and contralateral disease.
This can significantly alter the course of treatment,
from breast-conserving surgery to more extensive surgery or mastectomy.
Optimal MR imaging of the breasts requires T1-weighted sequences,
with fat suppression,
performed before and after administration of contrast material which maximize temporal and spatial resolution while minimizing section thickness.
The first phase is used as a subtraction mask,
with a subsequent pause during which images are checked and contrast material injection is initiated.
Following the intravenous bolus administration of gadolinium,
imaging in remaining phases are acquired continuously.
DCIS can be hypo- to isointense on precontrast T1-weighted and fat-saturated T2-weighted images.
The most commonly reported MR imaging manifestation of DCIS is clumped nonmasslike enhancement in a ductal,
linear,
segmental,
or regional distribution.
The most frequent enhancement pattern is clumped enhancement,
followed by heterogeneous,
homogeneous,
reticular,
and punctate.
High-grade DCIS more frequently manifests as an enhancing mass than does intermediate or low-grade DCIS.
Low-grade DCIS frequently shows non masslike enhancement or no enhancement.
Two distinct patterns of neovascularization may occur in DCIS: periductal and stromal.
The periductal pattern manifests as a dense rimlike network of micro-vessels adjacent to the basement membrane of a duct.
The stromal pattern is characterized by a more diffuse increase in vascularity of the stroma between DCIS lesions.
There is wide variability in the reported enhancement kinetic curve of DCIS,
with the most common pattern being early enhancement with plateau kinetics,
the plateau enhancement kinetic curve is more commonly seen than washout or progressive enhancement kinetics.
No kinetic pattern is pathognomonic of a particular nuclear grade of DCIS.
Thus,
the image interpretation and final recommendations should be based on the morphologic characteristics instead of the enhancement kinetics of the lesion.
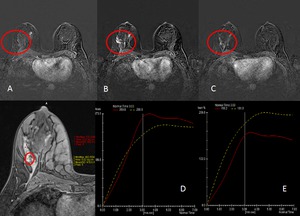
Fig. 5: Axial MR images obtained in a 52-year-old asymptomatic woman.
(A) T1WIs Precontrast (B ;C), early postcontrast, and late postcontrast enhanced fat-suppressed T1W fast spoiled gradient-echo MR images show multifocal segmental enhancing at right breast. (D,E,) kinetic curves with plateau enhancement kinetic curve
Usually DCIS lesions with a masslike appearance at mammography demonstrate strong washout at MR imaging,
whereas DCIS lesions that appeared as pleomorphic,
fine linear,
or fine linear-branching calcifications at mammography show plateau enhancement at MR imaging.
Furthermore,
DCIS lesions that appeared as amorphous calcifications at mammography exhibited persistent delayed enhancement.
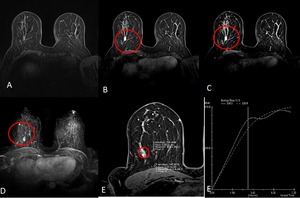
Fig. 6: Axial MR images obtained in a 47-year-old woman with a palpable mass in the right breast.
(A) T1WIs Precontrast (B ;C), early postcontrast, and late postcontrast enhanced fat-suppressed T1W fast spoiled gradient-echo MR images of the right breast show a focal enhancing at right breast. (D) Axial MIP reformated images (E) kinetic curves with plateau enhancement. Biopsy revealed high-grade DCIS.
Although second-look US can be used to identify MR imaging–detected malignant lesions,
it is better at detecting a correlate for enhancing masses than nonmass enhancement,
the most common enhancement type in DCIS.
In this case if no US correlate is identified for a suspicious area of non mass enhancement,
MR imaging–guided biopsy should be performed.
Because malignant features (eg,
spiculations,
angular margins,
echogenic halo,
and posterior shadowing) may be absent,
a lower threshold should be used at second-look US than at conventional diagnostic or screening US.

 as well as amorphous and fine pleomorphic calcifications (curved arrow) in the upper outer quadrant. B- US image demonstrates calcifications within ducts.
Stereotactic biopsy revealed high-grade DCIS")



 T1WIs Precontrast (B ;C), early postcontrast, and late postcontrast enhanced fat-suppressed T1W fast spoiled gradient-echo MR images show multifocal segmental enhancing at right breast. (D,E,) kinetic curves with plateau enhancement kinetic curve")
 T1WIs Precontrast (B ;C), early postcontrast, and late postcontrast enhanced fat-suppressed T1W fast spoiled gradient-echo MR images of the right breast show a focal enhancing at right breast. (D) Axial MIP reformated images (E) kinetic curves with plateau enhancement. Biopsy revealed high-grade DCIS.")