ECR 2013 / C-2369
Primary Appendiceal Neoplasms: Clinical, Pathologic and Imaging Analysis
Congress:
ECR 2013
Poster Number:
C-2369
Type:
Educational Exhibit
Keywords:
Diagnostic procedure, MR, CT, Oncology, Abdomen, Pathology
Authors:
E. M. Abreu1, M. A. E. C. Vasconcelos2, N. V. V. B. Marques3, M. Palmeiro1, J. Niza2, A. Loureiro2, R. Canas Marques1, S. Vinhais2; 1Lisbon/PT, 2Lisboa/PT, 3Carcavelos/PT
DOI:
10.1594/ecr2013/C-2369

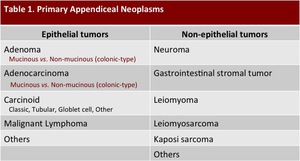
Table 1:
Classification of primary appendiceal neoplasms.

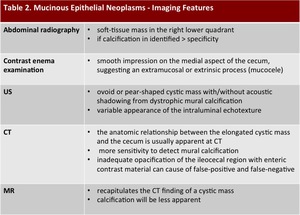
Table 2:
Imaging features of mucinous epithelial neoplasms of the appendix.
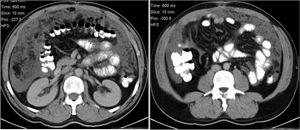
. The adjacent mesenteric fat has an increased density, due to coexistent inflamation. Macroscopy is shown. The hystological analysis revealed a mucinous cystadenoma with coexistent mucocele and inflamation.")
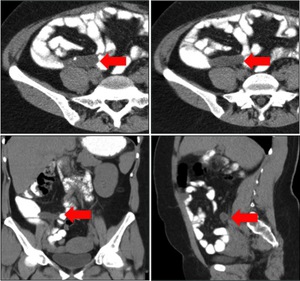
Fig. 1:
Mucocele from mucinous cystadenoma of the appendix. Axial contrast-enhanced CT...
 in the expected region of the appendix, which measures 46x18x14mm. An eccentric calcification is seen. Coronal and sagital CT images show the same radiological findings (red arrow).")
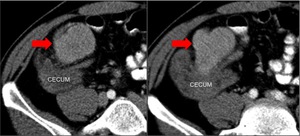
Fig. 2:
Mucocele from mucinous adenocarcinoma of the appendix. Axial CT scan shows an...
 in the expected region of the appendix, findings that represent a primary mucinous adenocarcinoma of the appendix, confirmed by the histological analysis.")
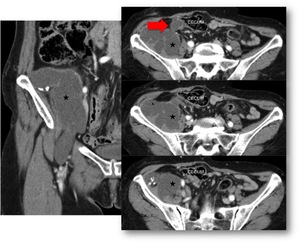
Fig. 3:
Mucocele from mucinous adenocarcinoma of the appendix. Different levels of an...
. Coronal CT image also demonstrates a soft-tissue mass in relation to peritoneal implants (black star).")
Fig. 4:
Metastatic mucinous adenocarcinoma of the appendix. Axial and sagital...

Fig. 5:
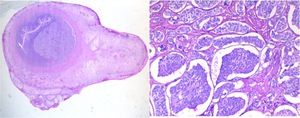
Mucinous adenocarcinoma of the appendix. Hematoxylin and eosin stain. Low power...
.")
Fig. 6:
Pseudomyxoma retroperitonei from mucinous adenocarcinoma of the appendix....
 and a lobulated hypoattenuating mass with tiny wall calcifications. The mass is observed in the right retroperitoneal space and displaces the adjacent structures, infiltrating the right iliac muscle (black star). Note the mass extension into the right crural canal. A CT guided biopsy confirmed the diagnosis.")
Fig. 7:
Pseudomyxoma retroperitonei from mucinous adenocarcinoma of the appendix. Axial...
 and a lobulated hypoattenuating mass in the right retroperitoneal space that displaces the adjacent structures, infiltrating the right iliac muscle (black star). Note the mass extension into the right crural canal. A CT guided biopsy confirmed the diagnosis.")
Fig. 8:
Pseudomyxoma retroperitonei from mucinous adenocarcinoma of the appendix....

Fig. 9:
Pseudomyxoma peritonei from mucinous adenocarcinoma of the appendix manifesting...

Fig. 10:
Colonic-type adenoma of the appendix. Different levels of an axial CT in a...
 found incidentally, in the proximal region of the appendix. Pathological analysis revealed a poor differentiated serous adenocarcinoma.")
Fig. 11:
Colonic-type adenocarcinoma of the appendix. Axial contrast-enhanced CT scan...
 of the appendix. Axial contrast-enhanced CT scan shows an elongated structure that corresponds to the appendix vermiform (red arrow). Note the presence of multiple peri-appendicular lymph nodes. Hystological analysis demonstrated a carcinoide tumor with 1cm in diameter, located in the caudal region of the appendix, that involves all parietal layers.")
Fig. 12:
Neuroendocrine tumor (classic carcinoid) of the appendix. Axial...
 of the appendix. SPECT detected pathological emitted radiation in in the expected region of the appendix.")
Fig. 13:
Neuroendocrine tumor (classic carcinoid) of the appendix. SPECT detected...
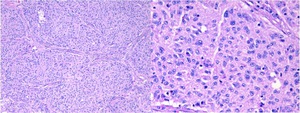
 of the appendix. Hematoxylin and eosin stain. Low power magnification view and 200x magnification view.")
Fig. 14:
Neuroendocrine tumor (classic carcinoid) of the appendix. Hematoxylin and eosin...

Fig. 15:
Follicular Dendritic Cell Sarcoma. Axial contrast-enhanced TC scan, performed...

Fig. 16:
Follicular Dendritic Cell Sarcoma infiltrating the appendix parenchyma....
.")
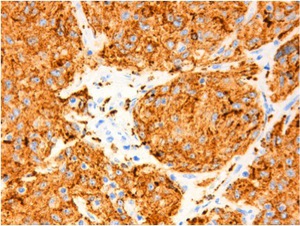
Fig. 17:
Follicular Dendritic Cell Sarcoma. The neoplastic cells are immunoreactive with...