ECR 2013 / C-2504
Abnormal flow dynamics within the ascending aorta of the patients with aortic valve stenosis. Assessments with phase resolved three dimensional phase contrast MR image (4D-Flow).
Congress:
ECR 2013
Poster Number:
C-2504
Type:
Scientific Exhibit
Keywords:
Dilatation, Imaging sequences, Computer Applications-3D, MR-Angiography, MR, Cardiovascular system, Arteries / Aorta, Aneurysms
Authors:
M. Sugiyama1, Y. Takehara1, T. Saito1, N. Ooishi1, M. Alley2, T. Wakayama3, M. Terada4, S. Yoshihara4, H. Sakahara1; 1Hamamatsu/JP, 2Stanford, CA/US, 3Hino/JP, 4Iwata/JP
DOI:
10.1594/ecr2013/C-2504
 at systole.
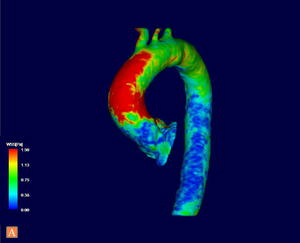
The WSS of the dilated ascending aorta is reduced due to the complex abnormal flow dynamics.")
Fig. 3:
The WSS of an AS patient (the same case as Fig.1) at systole.
The WSS of the...
.
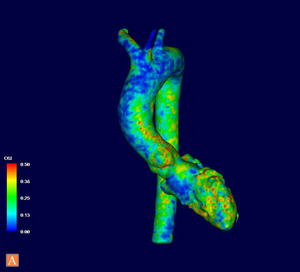
Higher OSI is seen on the wall nearby the complex abnormal flow dynamics.")
Fig. 7:
The OSI of an AS patient (the same case as Fig.1).
Higher OSI is seen on the...
.
WSS is homogeneously high at the ascending aorta compared to the AS patients.")
Fig. 4:
The WSS at systole of a control case (the same case as Fig.2).
WSS is...
.
The calculated OSI of the control group shows stable and low OSI compared to the AS patients.")
Fig. 8:
The OSI of a control case (the same case as Fig.2).
The calculated OSI of the...
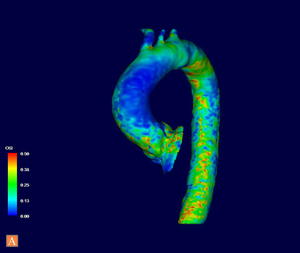
. Higher OSI is still seen at base of the ascending aorta.")
Fig. 9:
Partially lower OSI was observed at the dilated ascending aorta in a...
.")
Fig. 5:
Partially high WSS is depicted in the ascending aorta at systole within a...

Fig. 10:
The formula for OSI calculation.