Schematic animations,
illustrations,
CT angiograms and MRI aniograms are used to illustrate development,
anatomy and variants of cerebral arteries.
Normal variations include fenestrations,
duplications,
variants of the circle of Willis,
persistent carotid-basilar anastomoses,
and other vascular anomalies in the skull base.
When assessing CT or MRI angiograms,
it is important to think about normal variants,
their prevalence,
and their clinical relevance,
particularly with respect to the risk of aneurysm formation or surgical complications.
Imaging of variations:
There are some anomalies which can be depicted in several arteries and they should be described at the beginning of the review - these include fenestrations,
duplications and infundibulum.
Fenestration is defined as a division of the arterial lumen into separate channels.
Various mechanisms have been proposed for development of different fenestrations.
Fenestrations of intracranial arteries are generally asymptomatic but similar to arterial bifurcations,
they have a tendency to develop aneurysms.
Duplication is defined as two arteries with separate origins and no distal arterial convergence.
Infundibulum it is funnel-shaped region of dilatation at the origin of the artery,
it must be distinguished from aneurysm.
Below these and other variations of circle of Willis arteries.
Anterior cerebral artery (ACA)
-
Median artery of corpus callosum (medial ACA,
median callosal artery,
superior callosal artery,
third A2 artery,
triplicated ACA,
ACA trifurcation,
accesory ACA)
Description: branch of the AcoA,
runs parallel to and behind the normal pericallosal artery; it is postulated that this variant results from persistence of embryonic MACC or marked development of MACC because of hypoplastic ACA.
Clinical significance: frequently encountered as one of the draining arteries of the ACoA aneurysm,
it can be difficult to identify such aneurysms,
depending on their orientation,
and it is easy to damage them during surgery.
-
A1 Segment Absence or Hypoplasia
Description: absent or hypoplasia of A1 segment,
contralateral anterior cerebral artery may supply part or all of the territory of the normal anterior cerebral artery via anterior communicating artery.
Clinical significance: in the event of thromboembolic disease,
these conditions result in a diminished collateral supply and therefore an increased risk of infarction.
- Azygos (undivided,
unpaired) ACA:
Description: single midline vessel arising from the confluence of the A1 segment of ACAs,
represents persistence of the embryonic median artery of the corpus callosum.
Clinical significance: no direct evidence of any increased incidence of stroke associated with azygous ACA but occlusion can cause ischemic infarction in both cerebral hemispheres and the corpus callosum.
An azygous ACA can be associated with midline central nervous system malformations,
such as agenesis of corpus callosum,
holoprosencephaly,
intracranial arteriovenous malformation,
and aneurysm.
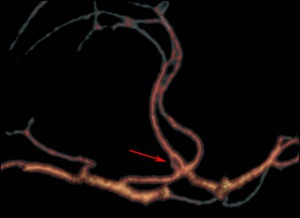
Fig. 2: Fenestrations of the anterior cerebral artery. CT angiogram shows dual channels arising from the origin of the A2 segment (arrow).

Fig. 3: Trifurcation of the anterior cerebral artery. MR angiogram shows three A2 segments (arrow).
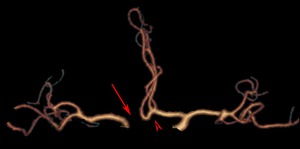
Fig. 4: Absence of an A1 segment of the anterior cerebral artery (arrow). CT angiogram shows also trifurcation of the anterior cerebral artery (arrowhead).
Anterior Communicating Artery (AcomA)
-
Fenestration,
Description: it is postulated that this anomaly is the remnant of the plexiform anastomosis between the two converging ACAs ,
ACOM is one of the most common sites of fenestration,
Clinical significance might be mistaken for ACoA aneurysm on MRA.
-
Duplication,
Description: each vessel originating separately from an anterior cerebral artery.
-
Absence
Description: the AcomA often is not depicted at angiography,
but this does not necessarily mean that the artery is absent.
Middle Cerebral Artery (MCA)
-
Duplication
Description: two vessels originating from the distal end of the ICA.
The duplicate vessel parallels the main MCA and supplies the anterior temporal lobe; it is postulated that this anomaly iderives from persistent anastomoses between the ACA and MCA.
Clinical significance: reports of aneurysms formation at the origin of a duplicate middle cerebral artery.
-
Accessory MCA,
Description: anomalous vessel originating from ACA,
which courses parallel to the M1 segment of the middle cerebral artery,
supplying the anterior-inferior region of the frontal lobe,
it is postulated that this anomaly derives from persistent anastomoses between the ACA and MCA.
Clinical significance: aneurysm formation.
-
Early branching
Description: Early division of the M1 segment close to its origin at the internal carotid artery.
Clinical significance: not associated with an increased risk of aneurysm formation.
-
Fenestrations
Description: Early branching temporopolar artery may participate in the formation of MCA fenestration.
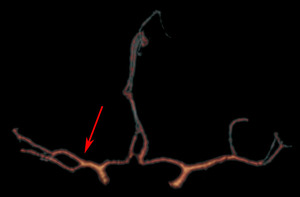
Fig. 5: Early branching of the middle cerebral artery. CT angiogram shows a unilateral early bifurcation of the right middle cerebral artery (arrow).
Posterior Cerebral Artery (PCA)
-
Fetal PCA,
Description: failing in regression of embryonic PCoA,
ipsilateral P1 segment may hipoplastic or absent.
Clinical significance: while treating the ICA–PCoA aneurysm,
fetal PCA should not be occluded to avoid infarction of the PCA territory.
-
Fenestration
Description: origin not clear.
-
Common Posterior Cerebral and Superior Cerebellar Artery Trunk
Description: common trunk of the superior cerebellar artery and P1 segment of the posterior cerebral artery.
Clinical significance: important in the surgery and endovascular treatment of the BA aneurysm.
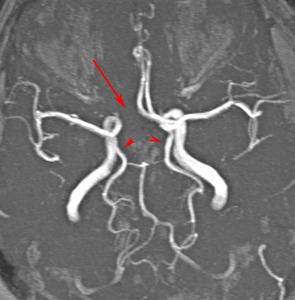
Fig. 6: MR angiogram shows A1 segment absence (arrow) and bilateral fetal posterior cerebral arteries (arrowheads).
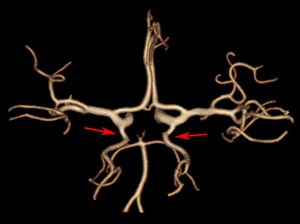
Fig. 7: Bilateral fetal posterior cerebral arteries (arrows) on CT angiogram. Both P1 segments are hipoplastic.
Posterior Communicating Artery (PcomA)
Vertebral Artery (VA)
-
Fenestration,
Description: extracranial fenestrations are probably caused by the persistence of cervical intersegmental arteries,
the intracranial components may arise from persistent basivertebral anastomoses or passage of a solid structure (such as the hypoglossal nerve).
Clinical significance: often associated with anomalies of the brain,
spinal cord,
and spine,
and with other vascular anomalies,
also reported an increased prevalence of aneurysms and vascular malformations.
-
Duplication
Description: very rare
Basilar Artery (BA)

Fig. 8: Basilar artery fenestration. CT angiogram shows fenestration at the origin of the basilar artery.
Hyperplastic Anterior Choroidal Artery
Description: usually a small vessel,
arises from the supraclinoid ICA just distal to the PcomA.
Anterior choroidal artery is described as hyperplastic when the temporo-occipital branches of the PCA arise from this vessel.

Fig. 9: CT angiogram shows hyperplastic anterior choroidal artery (white arrow), ipsilateral fetal posterior cerebral artery (red arrow), note also the trifurcation of the anterior cerebral artery (arrowhead).
Persistent primitive olfactory artery
Description: arises from the terminal portion of the ICA,
runs along the olfactory bulb,
makes an posterior turn behind the olfactory bulb,
and finally becomes the distal ACA.
Usually involutes to a remnant known as the recurrent artery of Heubner.
Persistance is associated with the absence of AComA and the recurrent artery of Heubner.
Clinical significance: high incidence of cerebral aneurysms.
Persistent Dorsal Ophthalmic Artery
Description: two primitive ophthalmic arteries are present: The ventral ophthalmic artery,
which normally persists,
and the dorsal ophthalmic artery,
which normally regresses.
In some instances,
the opposite situation occurs,
and the dorsal ophthalmic artery persists.
This variant artery arises from the dorsal aspect of the supraclinoid portion of the ICA and enters the orbit by way of the superior orbital fissure instead of the optic canal.
Presegmental Arteries and Carotid-basilar anastomoses:
Description: among all persistent carotidbasilar anastomoses,
persistent trigeminal artery (PTA) is the most common and most cephalic in location.
Clinical significance: persistent anastomoses may be associated with various vascular anomalies,
these include carotid-cavernous fistula,
aneurysms,
Sturge–Weber syndrome,
hemangioma of the head and neck,
cerebral arteriovenous malformations,
etc.
Persistance may be responsible for neuralgia or paralysis of associated cranial nerves.
Recognition of these variants also warrant appropriate modifications of interventional neuroradiology or endovascular procedures.
For example recognition of the PTA can be important in surgical procedures in the cavernous sinus or the posterior fossa,
and may prevent injury or disruption of the PTA.
Endovascular procedures should be modified accordingly to avoid ischemia to the brainstem and the cerebellum.
-
Persistent primitive trigeminal artery (PTA)
Description: artery named for its association with 5th nerve,
PTA arises from posterior genu of cavernous (C4) segment of ICA and joins the cephalic end of the basilar artery adjacent to the clivus - may follow either a parasellar (lateral to the dorsum) or intrasellar course.
PTA is classified into two types according to its course: a medial type in which the artery runs through the dorsum sellae and perforates the dura mater near the clivus,
and a lateral type in which the artery runs between the sensory root of the trigeminal nerve and the lateral side of the sellae and penetrates the dura mater medial to Meckel’s cave.
PTA is also classified according to configuration of other arteries into three types of patterns:
Saltzman type I – PTA joins basilar artery between the superior cerebellar arteries and anterior inferior cerebellar arteries.
The basilar artery proximal to the junction is usually hypoplastic and the posterior communicating arteries are absent or poorly opacified;
Saltzman type II - PTA joins the basilar artery between superior cerebellar arteries and anterior inferior cerebellar arteries,
but the posterior communicating arteries are present and supply the posterior cerebral arteries;
Saltzman type III - PTA directly joins to the cerebellar artery.
-
Persistent primitive hypoglossal artery (HA)
Description: artery named for its association with 12th nerve,
second most common after PTA,
persistent vessel arises from ICA at C1 to C3 segments,
enters the skull through anterior condylar or hypoglossal canal (not through the foramen magnum) and courses posteromedially to continue as terminal segment of the VA and BA.
The contralateral VA,
if present,
generally terminates in the posterior inferior cerebellar artery.
-
Persistent Otic Artery
Description: artery named for its association with 8th nerve,
existance of persristent OA in human is controvertial.
True otic artery must originate from lateral-most portion of the petrous segment of the ICA and then traverse through the internal auditory meatus before joining the caudal end of basilar artery.

Fig. 10: MR angiogram demonstrates lateral persistent trigeminal artery Saltzman type 1 (arrow). Note the hypoplastic vertebral artery (arrowhead).

Fig. 11: MR angiogram demonstrates lateral persistent trigeminal artery Saltzman type 1 (arrows). Note the hypoplastic vertebral artery (arrowhead).
Internal Carotid Artery (ICA)
-
Agenesis and hypoplasia
Description: improper developments of one of 7 different emryologic segments that form the ICA; may be congenital or acquired due to occlusion or stenosis respectively (key finding is the absence of petrous bony carotid canal in ICA agenesis and smaller size of the canal in ICA hypoplasia).
Clinical significance: unilateral absence generally asymtomatic,
in the presence of insufficuent collaterals may occur symptoms related to uncompensated blood flow,
intracranial aneurysms because of hemodynamic changes in collateral vessels has been described.
Congenital agenesis or hypoplasia of the internal carotid artery may be associated with anencephaly and basal telangiectasia.
-
Aberrant Internal Carotid Artery
An aberrant intratympanic ICA
Description: enters the floor of middle ear space (through an enlarged inferior tympanic canal that lies posterior to the normal carotid canal) instead of staying anterior to this space before entering the foramen lacerum and middle cranial fossa.
The normal vertical portion of the carotid is absent or hypoplastic and can be confused with dissection.
Pathology: due to agenesis or hypoplasia of ICA,
the inferior tympanic artery does not regress,
instead hypertrophies and anastomoses with the caroticotympanic artery to supply carotid siphon.
Clinical significance: asymptomatic or nonspecific symptoms such as conductive hearing loss,
pulsatile tinnitus,
ear fullness,
otalgia,
vertigo; middle ear vascular mass comon - danger of iatrogenic ear bleeding – if suspected it is crucial to inform clinician.
An abberant lateral pharyngeal ICA
Description: ICA extends to or near the midline posterior pharyngeal wall.
Pathology: ICA uncoils as the dorsal aortic root descends into the chest and finally assumes a stright course in the neck.
Clinical significance: recognition is crucial in preoperative diagnosis (before oropharyngeal tumor resection,
tonsillectomy,
adenoidectomy,
palatopharyngoplasty.
-
Fenestration
Persistent Stapedial Artery
Description: The stapedial artery is a normally transient anastomosis between the branches of the future external carotid artery and internal carotid artery.
The stapedial artery arises from the vertical part of the petrous internal carotid artery,
passes through the obturator foramen of the stapes,
and terminates as the middle meningeal artery.
Clinical significance: pulsatile tinnitus,
presence may complicate tympanotomy,
stapedectomy,
and cholesteatoma resection and prevent cochlear implantation.


. Note the hypoplastic vertebral artery (arrowhead).")
.")

 on CT angiogram. Both P1 segments are hipoplastic.")
 and bilateral fetal posterior cerebral arteries (arrowheads).")
. CT angiogram shows also trifurcation of the anterior cerebral artery (arrowhead).")
.")