CALCIFIC TENDINITIS OF THE ROTATOR CUFF
Etiology
The term “calcific tendinitis” refers to the intratendinous deposition of calcium,
predominantly hydroxyapatite,
that can affect every tendon in the body and especially the rotator cuff.
This pathological condition is a dynamic process that evolves through pre-calcific and calcific (formative,
resorptive,
reconstitutive) stages (Fig.1).

Fig. 1: Calcific stage:(a)Formative,(b)Resorptive,(c)Reconstitutive.
In the precalcific stage,
microtraumatic factors associated with a local decrease in blood supply can lead to intratendinous fibrocartilaginous metaplasia, with resulting calcification.
The subsequent formative phase is considered as a resting period.
Eventually,
triggered by unknown factors,
there is resorption of the deposit,
accompanied by vascular invasion,
the migration of phagocytic cells with dissolution of the calcific focus (resulting in a “toothpaste” appearance of the calcific deposit) and edema from intratendinous pressure, such that the condition becomes symptomatic.
After resorption,
in the reparative phase,
fibroblasts restore the normal tendinous collagen pattern.
Epidemiology
Rotator cuff calcific tendinitis is a commonly seen condition,
occurring in up to 20% of painful shoulders and up to 7.5% of asymptomatic shoulders.
It is more frequent in women in their 40s and 50s and seems not to be related to physical activity.
The supraspinatus tendon (80% of cases),
followed by the infraspinatus (15% of cases) and subscapularis (5% of cases) tendons, is the most commonly affected cuff tendon.
The lower third of the infraspinatus tendon,
the critical zone of the supraspinatus tendon,
and the pre-insertional fibers of the subscapularis tendon are the most frequently affected locations.
This condition is typically associated with an intact rotator cuff.
Clinical Presentation
The pre-calcific stage is usually asymptomatic.
The typical clinical manifestation is low-grade subacute pain that usually increases at night and corresponds to the calcific stage,
variably associated with mechanical symptoms according to the size of the deposit.
In many cases,
however,
rotator cuff calcific tendinitis can be a highly disabling disorder,
with sharp acute pain that limits shoulder movement and is resistant to high doses of oral anti-inflammatory drugs.
This clinical presentation usually coincides with the resorptive stage; fever,
reflecting rupture of the calcification into the adjacent structures,
is occasionally reported.
However,
the acute phase of calcific tendinitis of the rotator cuff is regarded as a selfhealing condition,
with spontaneous resolution in 7–10 days.
Ultrasound Diagnosis
Three types of calcifications have been described: type I consists of a hyper-reflexive lesion with a well-circumscribed dorsal acoustic shadow; type II deposits are well-circumscribed,
homogeneous hyperechoic foci with a faint posterior shadow; type III are amorphous,
inhomogeneous hyperechoic foci without posterior acoustic shadow (Fig.2).
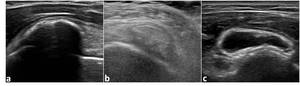
Fig. 2: Calcifications: (a) Type I, (b) Type II, (c) Type III.
The consistency is solid for deposits of types I and II and semi-liquid for type III calcifications.
Treatment Options
Asymptomatic cases usually do not require treatment, as the process is self-healing.
In patients with mild symptoms,
the disease can be managed conservatively with physical therapy and a short course of oral NSAIDs. Lithotripsy is only partially effective.
An alternative therapeutic approach is to extract the calcific material in an arthroscopy or imaging-guided procedure.
Imaging-guided treatments:
- fluoroscopy;
- ultrasound guided single or double needle technique.
PURPOSE OF THE STUDY
US-guided percutaneous treatment of RCCT has been demonstrated to be effective using one or two needles,
but direct comparison between the two methods has never been performed.
Our aim was to compare the technical and one-year clinical outcome of these two approaches.

Formative,(b)Resorptive,(c)Reconstitutive.")
 Type I, (b) Type II, (c) Type III.")