ECR 2014 / B-0048
Ultrasound-guided percutaneous injection for De Quervain’s disease using three different techniques: preliminary results of a randomised controlled trial
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2014
Poster Number:
B-0048
Type:
Scientific Paper
Keywords:
Musculoskeletal soft tissue, Ultrasound, Puncture, Inflammation
Authors:
D. Orlandi1, G. Ferrero1, E. Fabbro1, G. Serafini2, E. Silvestri1, L. M. Sconfienza3; 1Genoa/IT, 2Pietra Ligure/IT, 3San Donato Milanese/IT
DOI:
10.1594/ecr2014/B-0048

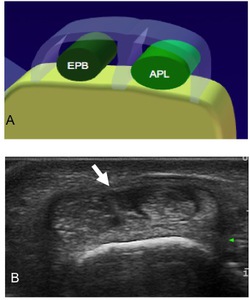
Fig. 2:
Schematic draw of wrist compartments involved in De Quervain's disease
 and US scan of a vertical septum (arrow) between extensor pollicis brevis (EPB) and abductor pollicis longus (APL).")
Fig. 3:
Schematic draw (A) and US scan of a vertical septum (arrow) between extensor...

Fig. 4:
Finkelstein's Test
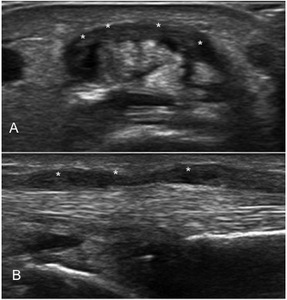
 and long axis (B) US scan of the first dorsal compartment of the wrist showing marked retinaculum thickening (asterisks).")
Fig. 5:
Short axis (A) and long axis (B) US scan of the first dorsal compartment of the...