CHOICE OF IMAGING MODALITY
- Radiography should initially be performed to diagnose or rule out acute osseous injury,
such as fractures and dislocations
- Radiographically occult fractures may be detected using CT or MRI,
if clinically suspected
- Muscle,
tendon and ligamentous injuries can be initially diagnosed using ultrasound.
For injuries of deep structures or large/extensive lesions,
MRI can depict a larger region of interest,
with more detailed anatomical information of the type and extent of lesion
Neck Injuries:
- Cervical Spine Fracture and C5 Nerve Root Injury
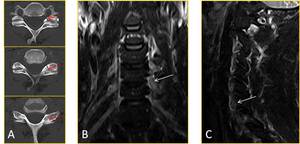
Fig. 3: 46-year-old male semi-professional mountain biker sustained a high speed fall on a downhill. Axial CT images (A) show a non-displaced fracture of the left C6 facet (red arrows). Coronal (B) and sagittal (C) STIR images show left C5 nerve root thickening with abnormal hyperintensity (white arrows), compatible with neuropraxia.
References: Dept. of Radiology, Boston University School of Medicine, Boston, USA, and Van Wageningen and Partners, Somerset West, South Africa 2014
Shoulder/Thorax Injuries (1):
- Scapular Fracture and Pneumothorax
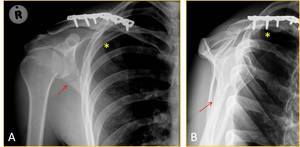
Fig. 4: 36-year-old male mountain biker who developed right shoulder pain and shortness of breath following a fall during a competition. Frontal (A) and Y-view (B) radiographs of the right shoulder show orthopaedic hardware from prior ORIF of the right claviclular fracture and right apical pneumothorax (*). A new aligned and non-displaced right scapular fracture (red arrows) is also seen.
References: Dept. of Radiology, Boston University School of Medicine, Boston, USA, and Van Wageningen and Partners, Somerset West, South Africa 2014
Shoulder/Thorax Injuries (2):
- Clavicular Fracture,
Rib Fractures and Humeral Avulsion Fracture
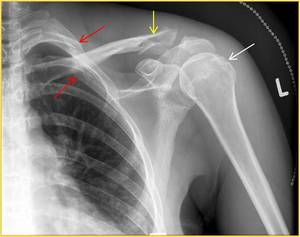
Fig. 5: 37-year-old female mountain biker who fell from her bike during a competition. She developed left shoulder and chest pain, as well as painful proximal left upper arm with inability to move her left shoulder due to pain. Frontal radiograph of the left shoulder shows communited distal third claviclular fracture (yellow arrow), 2nd and 3rd rib fractures (red arrows), and probable avulsion fracture of the greater tuberosity of the humerus (white arrow).
References: Dept. of Radiology, Boston University School of Medicine, Boston, USA, and Van Wageningen and Partners, Somerset West, South Africa 2014
Shoulder/Thorax Injuries (3):
- Clavicular Fracture with Incidental Pneumonitis
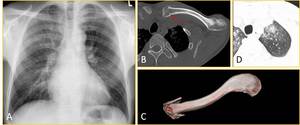
Fig. 6: 38-year-old male mountain biker who developed left shoulder pain and shortness of breath following a fall during a competition. Frontal radiograph (A) incidentally shows increased interstitial markings in the bilateral lungs. Axial CT image in bone window (B) and 3D reconstructed image (C) show impacted left proximal third clavicular fracture (red arrow). Axial CT image in lung window (D) also demonstrates insterstitial densities bilaterally, which was thought to represent hypersensitivity pneumonitis, likely secondary to dust inhalation. Follow-up radiograph 14 days later was normal.
References: Dept. of Radiology, Boston University School of Medicine, Boston, USA, and Van Wageningen and Partners, Somerset West, South Africa 2014
Shoulder Injuries:
- Posterior Glenoid Labral Tear
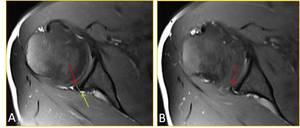
Fig. 7: 32-year-old male mountain biker presented with 1-month history of persistent right shoulder pain following a fall on an outstretched hand during a competition 1 month ago. Axial T2-weighted fat-saturated images (A & B) demonstrates the right posterior glenoid labral tear (red arrows) with a small paralabral cyst (yellow arrow).
References: Dept. of Radiology, Boston University School of Medicine, Boston, USA, and Van Wageningen and Partners, Somerset West, South Africa 2014
Forearm Injuries (1):
- Nightstick Fracture

Fig. 8: 21-year-old male mountain biker presented with acute right forearm pain after hitting the right forearm against a tree whilst on a single track. AP (A) and lateral (B) radiographs show an isolated fracture of the middle third of the right ulna (yellow arrows). Mechanism of injury: direct blow to the ulnar side of the forearm.
References: Dept. of Radiology, Boston University School of Medicine, Boston, USA, and Van Wageningen and Partners, Somerset West, South Africa 2014
Forearm Injuries (2):
- Retained Foreign Body
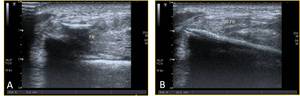
Fig. 9: 50-year-old male mountain biker who was flung off his mountain bike and landed in bushes, sustaining a penetrating injury. Despite repeated surgical explorations, the patient had persistent swelling of the right forearm. Ultrasound imaging demonstrated presence of two linear echogenic objects within the right forearm (A and B). Surgical exploration revealed retained wooden foreign bodies.
References: Dept. of Radiology, Boston University School of Medicine, Boston, USA, and Van Wageningen and Partners, Somerset West, South Africa 2014
Wrist Injuries (1):
- Occult Scaphoid Fracture
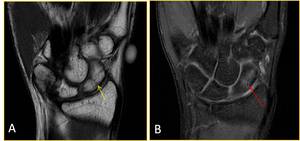
Fig. 10: 20-year-old male mountain biker presented with 2-month history of persistent right wrist pain following a fall during a competition. Radiograph of the right wrist at the time of injury was normal. Coronal T1-weighted image taken 2 months after injury (A) shows linear hypointensity within the body of scaphoid (yellow arrow), and coronal T2-weighted fat-saturated image (B) demonstrates ill-defined hyperintensity within scaphoid, consistent with occult scaphoid fracture without evidence of osteonecrosis (red arrows).
References: Dept. of Radiology, Boston University School of Medicine, Boston, USA, and Van Wageningen and Partners, Somerset West, South Africa 2014
Wrist Injuries (2):
- Occult Chauffeur Fracture

Fig. 11: 19-year-old male mountain biker presented acute right wrist pain following a fall during a competition. Oblique (A) and lateral (B) radiographs of the right wrist show a fracture through the distal radius involving the radial styloid process, consistent with Frykman type III fracture (Chauffeur fracture). Coronal T1-weighted image (C) shows linear hypointense fracture line in the distal radius (yellow arrow), and coronal T2-weighted fat-saturated image (D) demonstrates bone marrow edema around the fracture. Mechanism of injury: either from direct trauma, typically a blow to the dorsal side of the wrist or from forced dorsiflexion and abduction.
References: Dept. of Radiology, Boston University School of Medicine, Boston, USA, and Van Wageningen and Partners, Somerset West, South Africa 2014
Buttock Injuries (1):
- Ischial Bursitis

Fig. 12: 41-year-old female mountain biker presented with persistent left buttock pain with symptoms of left-sided sciatic nerve irritation. Ultrasound images demonstrate left-sided ischial bursitis.
References: Dept. of Radiology, Boston University School of Medicine, Boston, USA, and Van Wageningen and Partners, Somerset West, South Africa 2014
Buttock Injuries (2):
- Gluteal Tear with Haematoma
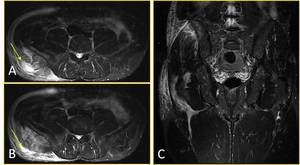
Fig. 13: 37-year-old male mountain biker presented with persistent right buttock pain following a fall on the right side. Axial (A&B) and coronal (C) MR images show ill-defined hyperintensity on T2-weighted fat-saturated images representing muscule oedema with a focal fluid collection representing haematoma (yellow arrows) in the right gluteal muscle.
References: Dept. of Radiology, Boston University School of Medicine, Boston, USA, and Van Wageningen and Partners, Somerset West, South Africa 2014
Buttock Injuries (3):
- Cyclist’s Nodule
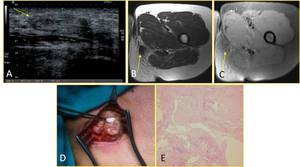
Fig. 14: 37-year-old female presented with 1-year history of persistent dull ache in the left inner buttock. Ultrasound (A) showed Well circumscribed predominantly hypo-echoic 2 x 1 cm nodule in the subcutaneous tissue just medial to the ischial tuberosity. Axial T1-w (A) and STIR (C) MR images show a hypo-intense lesion in close relation to the ischial tuberosity and proximal insertion of the hamstring. Surgical excision (D) and histology (E) confirmed a combination of fibrosis, oedema and cystic areas compatible with a cyclist nodule.
References: Dept. of Radiology, Boston University School of Medicine, Boston, USA, and Van Wageningen and Partners, Somerset West, South Africa 2014
Hip Injuries (1):
- Anterior Labral Tear
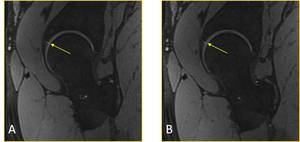
Fig. 15: 36-year-old male mountain biker presented with persistent right hip pain after long rides. Sagittal T2-weighted fat-saturated images demonstrate a tear of the anterior labrum (yellow arrows).
References: Dept. of Radiology, Boston University School of Medicine, Boston, USA, and Van Wageningen and Partners, Somerset West, South Africa 2014
Hip Injuries (2):
- Adductor Magnus Tear
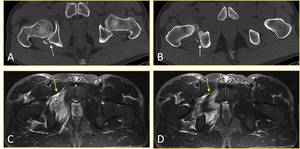
Fig. 16: 40-year-old male mountain biker presented with acute low back pain and right-sided hip pain after hitting an unexpected dip while riding a downhill single track in the dark. Axial CT image (A&B) shows comminuted right posterior acetabular fracture (white arrows. Axial T2-weighted fat-saturated images (C&D) demonstrate a tear of the right adductor magnus (yellow arrows). The patient also sustained fractures of the left L2 and L3 transverse processes (not shown).
References: Dept. of Radiology, Boston University School of Medicine, Boston, USA, and Van Wageningen and Partners, Somerset West, South Africa 2014
Thigh Injuries (1):
- Morel-Lavallée Lesion
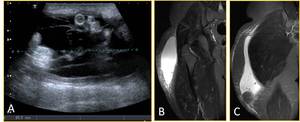
Fig. 17: 18-year-old male mountain biker presented with a large swelling of the right proximal thigh following a fall during a competition. Ultrasound image (A) demonstrates the presence of a large fluid collection. Coronal T2-weighted fat-saturated images (B and C) show a large subcutaneous seroma in the right thigh, consistent with Morel-Lavallée lesion.
References: Dept. of Radiology, Boston University School of Medicine, Boston, USA, and Van Wageningen and Partners, Somerset West, South Africa 2014
Thigh Injuries (2):
- Myositis Ossificans
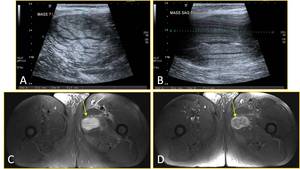
Fig. 18: 56-year-old male presented with 3 week history of left thigh pain after first-time mountain biking. Ultrasound (A and B) showed large, heterogeneous predominantly hyperechoic intramuscular mass within the medial aspect of proximal left thigh. Contrast-enhanced T1-weighted fat-saturated MR images showed a mass with heterogeneous enhancement in the left adductor magnus muscle (yellow arrows). Diagnosis of myositis ossificans was confirmed by biopsy.
References: Dept. of Radiology, Boston University School of Medicine, Boston, USA, and Van Wageningen and Partners, Somerset West, South Africa 2014
Thigh Injuries (3):
- Hamstring Avulsion Injury
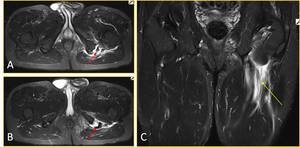
Fig. 19: 63-year-old male presented with acute left buttock/proximal thigh pain after jumping onto his mountain bike.3 week history of left thigh pain after first-time mountain biking. Axial (A and B) and coronal T2-weighted fat-saturated MR images showed avulsion injury of the left hamstrings at the ischial attachment (red arrows) and surrounding haematoma. Retraction of the proximal fibers (yellow arrow) with a bony fragment is seen.
References: Dept. of Radiology, Boston University School of Medicine, Boston, USA, and Van Wageningen and Partners, Somerset West, South Africa 2014
Knee Injuries:
- Occult Patellar Fracture Secondary to Patellar Dislocation
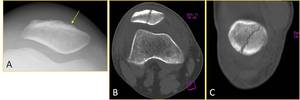
Fig. 20: 51-year-old male presented with 2 month history of right knee pain after sustaining a fall on the right knee during mountain biking. Skyline view radiograph (A) demonstrates subtle cortical disruption at the anterior surface of the patella (yellow arrow), while axial (B) and coronal reconstruction CT images (C) clearly show an oblique fracture without evidence of union.
References: Dept. of Radiology, Boston University School of Medicine, Boston, USA, and Van Wageningen and Partners, Somerset West, South Africa 2014
