Patients
This study was approved by the Institutional Review Board of Soonchunhyang University Bucheon Hospital.
The data from 358 patients who underwent gastrectomy for primary gastric cancer at our hospital between January 2010 and September 2012 were reviewed.
Classification of LN groups based on anatomical locations
LN groups can be divided roughly into perigastric LN and extra-perigastric (EP) LN groups.
However,
because the stomach has lesser curvature (LC) and greater curvature (GC) sides,we divided perigastric LNs into two groups: LC (#1,
3,
and 5 according to the Japanese classification) and GC (#2,
4sa,
4sb,
4d,
6,
and omentum).
The remaining LNs which were located EP area (except para-aortic area) was classified as the EP group.
Regardless of the number of metastatic LNs,
if any metastatic LN was involved in one group,
we considered the corresponding group is as positive for metastasis.
Finally,
we stratified the status of LN groups into four categories: 1) no metastatic LN in any groups was categorized as new N0,
2) if there was one positive among three groups (positive LC alone,
positive GC alone,
or positive EP alone),
regardless of number,
it was categorized as new N1,
3) if there were two positive out of three groups (positive LC + GC,
positive LC + EP,
or positive GC + EP),
regardless of number,
it was grouped as new N2,
and 4) if all three groups were positive (LC + GC + EP),
it was defined as new N3.
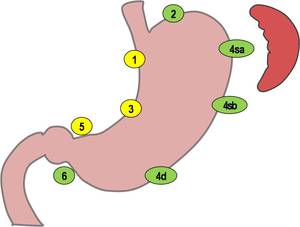
Fig. 1: Classification of lymph node groups based on anatomical location.Lesser curvature group (station number 1, 3, and 5, according to Japanese classification), and Greater curvature group (station number 2, 4sa, 4sb, 4d, 6).
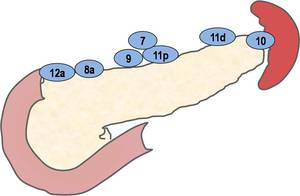
Fig. 2: Classification of lymph node groups based on anatomical location. Extra-perigastric group(except para-aortic area).
Image Analysis
CT images were independently reviewed by two experienced abdominal radiologists (M.H.L.
and H.K.L.
with 2- and 30-year experiences,
respectively) who were blinded to the endoscopic and the pathologic findings.
LNs were considered to be involved by metastasis if they were larger than 8mm in the short-axis diameter.
Each radiologist assessed LN metastasis twice according to the pN staging system,
the 7th edition of tumor-node-metastasis (TNM) from UICC and the new N staging with 1-week intervals to avoid the memory bias.
Statistical analysis
The diagnostic accuracy was calculated by comparing MDCT with the histopathological findings.
Inter-observer agreement for the current N staging and the new N staging was assessed with the weighted statistic.
The k values were interpreted as suggested by Landis and Koch.
where less than 0.00 indicated poor agreement,
0.00–0.20 indicated slight agreement,
0.21–0.40 indicated fair agreement,
0.41–0.60 indicated moderate agreement,
0.61–0.80 indicated substantial agreement,
and 0.81–1.00 indicated almost perfect agreement.
All statistical tests were performed with commercial software (STATA,
release 11; Stata Corp,
College Station,
Tex).

, and Greater curvature group (station number 2, 4sa, 4sb, 4d, 6).")
.")