Chest radiography is an important method for evaluating the diaphragm,
being the first imaging method which can give information regarding normal positioning and morphological changes,
and determining whether or not further evaluation is needed.
CT is,
without any doubt,
important for a more detailed evaluation of the diaphragm and any underlying condition which can cause changes in its normal position or morphology.
It can also help depict with more accuracy the normal anatomy.
This iconographic revision will focus mainly on common diaphragmatic pathology,
such as disfunction (eventration),
hernias and tumors,
which can be adequately seen with chest radiography and characterized with CT.

Fig. 18
EVENTRATION
It represents a congenital thinning of the diaphragm,
which leads to a focal bulge.
It usually only envolves a segment of the diaphragmatic dome,
frequently the anteromedial portion of the right dome.
It can become more pronounced with increased intra-abdominal pressure.
On chest radiography,
a portion of the hemidiaphragm is elevated,
while the rest remains at normal height.
At CT,
there's a sharp transition between the edges of the eventration.

Fig. 19: Chest Radiography PA view - Eventration. 54 year-old male patient with a focal elevation of the left diaphragmatic dome. This patient had a know history of cirrhosis and ascites.

Fig. 20: Chest Radiography lateral view - Eventration. 54 year-old male patient with a focal elevation of the left diaphragmatic dome. This patient had a know history of cirrhosis and ascites.
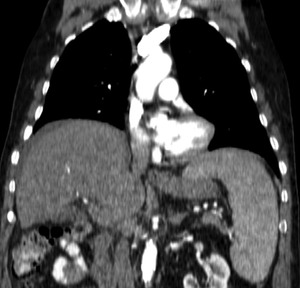
Fig. 21: CT coronal image - Eventration. 65 year-old patient who underwent CT for staging of colon cancer. Notice the right dome in an elevated position and the focal thinning of the hemidiaphragm in the antero-medial portion of the dome.
PARALYSIS AND WEAKNESS
There are many causes of paralysis and weakness of the diaphragm (Fig.16 - table PW),
which can be temporary of permanent depending on the cause.
Some can envolve the entire neuromuscular axis.
Phrenic nerve dysfunction is probably one of the most frequent causes of diaphragmatic paralysis or weakness encountered by the radiologist.
There are a multitude of causes for this impairment,
such as cardiac surgery,
radiation therapy,
tumors and neuropathies (Lyme's disease,
Guillain-Barré).

Fig. 22: Chest Radiography PA view - 62 year-old female patient with lung cancer. Notice the left apical pulmonary mass and ipsilateral elevation of the left diaphragmatic dome, secondary to invasion and paralysis of the left phrenic nerve.

Fig. 23: Chest Radiography lateral view - 62 year-old female patient with lung cancer. There's a continuous elevation of the left diaphragmatic dome, with no focal bulging, secondary to invasion and paralysis of the left phrenic nerve.
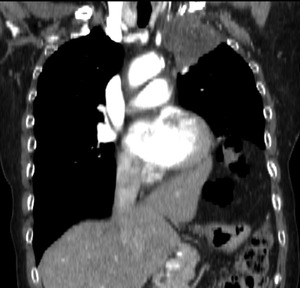
Fig. 24: CT coronal image - 62 year-old female patient with lung cancer. There's no clear plane between the pulmonary mass and the anterior thoracic wall and first rib, which suggests invasion of these structures.

Fig. 25
HIATAL
Hiatal hernias correspond to herniation of a portion of the stomach into the mediastinum,
through the esophageal hiatus.
There are essentially three types of hiatal hernias:
1)sliding hernia - the gastroesophageal junction and part of the stomach move into the thorax through and enlarged foramen.
2)paraesophageal hernia - the gastroesophageal junction remains in its normal position and a portion of the stomach herniates through the esophageal hiatus,
in an anterior position
3) congenital short esophagus - the stomach has a fixed position inside the thorax.
This type of hernia is more frequent in children.
Paraesophageal hernias are more prone to complications,
such as organoaxial volvulus of the stomach and colonic herniation.
Although most are congenital,
they can also be aquired,
namely after Nissen fundaplication.

Fig. 26: Chest radiography PA view - 40 year-old male patient with complaints of gastroesophageal reflux and halitosis. Notice the air-fluid level projected at the cardiac silhouette and the absence of gastric bubble. These findings are compatible with a hiatal hernia.
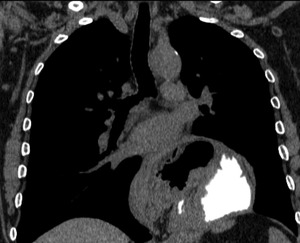
Fig. 27: CT coronal image - Hiatal hernia. Same patient as above. The MPR clearly depicts the gastroesophageal transition in the thorax and there is oral contrast within the herniated stomach.
MORGAGNI
The foramen of Morgagni (Fig.1 and Fig.2) is an anterior opening in the diaphragm,
which extends between the sternum medially and the 8th rib laterally.
Hernias occuring at this level are mostly unilateral and as much as 90% are right-sided.
In adulthood,
they can be an incidental finding after GI tract obstruction of pulmonary infection.
The most frequent finding on chest radiography is herniated bowel loops on a lateral view.
Other viscera can also herniate through the foramen of Morgagni,
such as liver,
spleen and omentum,
and CT is the preferred method of evaluation in these cases.

Fig. 28: Chest radiography PA view - 52 year-old female with incidintal finding of heterogeneous opacity, with some central foci of air, which occupies the lower right hemithorax. The patient underwent CT which demonstrated herniated bowel and omentum, findings compatible with Morgagni hernia.
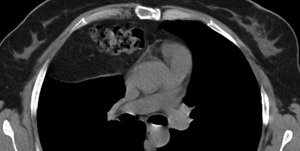
Fig. 29: CT axial image - Same patient as above. Notice the herniated colon and omentum. This is a typical finding for Morgagni hernias.
BOCHDALEK
This is a congenital hernia that occurs through a posterolateral defect in the diaphragm.
It is thought to arise from a malformation of the pleuroperitoneal fold or delay in the fusion of the pleuroperitoneal fold and transverse septum.
Most Bochdalek hernias are diagnosed in the antenatal period,
with a smaller number of patients manifesting respiratory distress after birth or being completelly assymptomatic in adulthood.
As much as 80% occur on the left side.
Associated anomalies are frequent in patients with Bochdalek hernias,
such as cardiovascular anomalies (ventricular or atrial septal defects,
Fallot tetralogy),
central nervous system defects and miscellanous conditions (cryptorchidism and cleft palate).
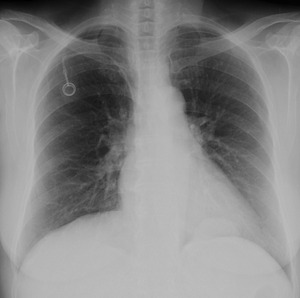
Fig. 30: Chest radiography PA view - 46 year-old female patient with breast cancer. The patient had complaints of dyspnea and there is an incidental finding of a homogeneous oval opacity in the lower and posterior left hemithorax. The patient underwent CT which revealed herniated fat in a small Bochdalek hernia.

Fig. 31: CT axial image - Bochdalek hernia. Same patient as above. There is a small herniation of fat through a posterolateral defect in the left hemidiaphragm.
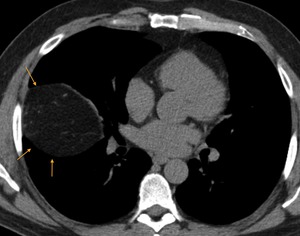
Fig. 32: CT axial image - Right Bochdalek hernia. Although more frequent on the right, as much as 20% of these hernias occur at the right hemidiaphragm.

Fig. 33
Diaphragmatic tumors are uncommon,
with scarse cases reported in the literature.
They occur with the same frequency in both men and women and exhibit the same prevalence in either right or left diaphragmatic leaflets.
When symptomatic,
there are more frequently associated with thoracic rather than abdominal symptoms,
namely dyspnea.
PRIMARY TUMORS
Primary diaphragmatic tumors are usually seen in a pediatric population,
and are malignant in 78% of the cases,
with rhabdomyosarcoma being the most frequent.
Other malignant tumors reported in the diaphgram are undifferentiated sarcomas and Ewing sarcoma and germ cell tumors in children.
Benign lesions can also be seen and the most frequent are lymphangiomas,
hemangiomas,
lipomas and myofibromas.
Cystic lesions are also uncommon and,
as primary tumors,
they're more frequent in children.
The most frequently described lesions are mesothelial cysts,
bronchogenic cysts and cystic teratoma.

Fig. 34: Chest radiography PA view - 7 year-old male patient with progressive dyspnea. Notice the marked deviation of the mediastinum and heart to the right due to a large mass that occupies the entire left hemithorax.
References: Centro Hospitalar e Universitário de Coimbra - Hospital Pediátrico
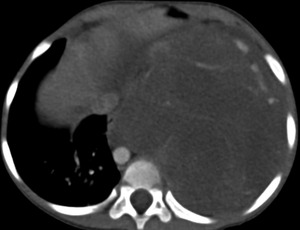
Fig. 35: CT axial image of the thorax - Same patient as above. There is an heterogeneous enhancing mass that the deviates the heart and mediastinal structures, with an unclear point of origin. The patient underwent surgery and was diagnosed with a diaphragmatic rhabdomyosarcoma.
References: Centro Hospitalar e Universitário de Coimbra - Hospital Pediátrico
SECONDARY TUMORS
Metastatic involvement of the diaphragm is quite rare,
with few reports in the literature.
It is usually seen in disseminated disease and can occur either by hematogenic spread or direct invasion.
The most frequent metastatic implants are secondary to head and neck tumors,
lung tumors and less frequently to colorectal cancer,
melanoma and breast cancers.
Neurogenic tumors have also been described,
and tend to involve the retrocrural space and diaphgramatic crura.

Fig. 36: CT axial image - 70 year-old male patient with complaints of abdominal pain. There is a large heterogeneous mass after contrast enhancement, predominantly hipodense with peripheral areas of vascularization, with unclear point of origin.
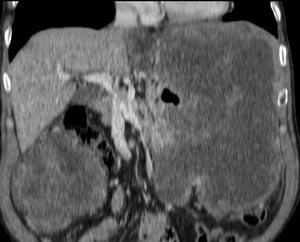
Fig. 37: CT coronal image - Same image as above. This mass seems to arise from the stomach, which has lost its normal morphology, and has a synchronous mass on the right flank. The patient underwent surgery and pathology revealed this was a gastric GIST with diaphgramatic infiltration.
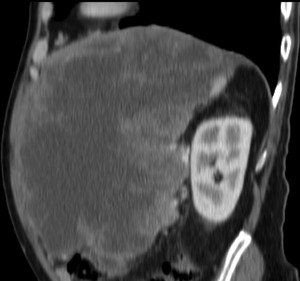
Fig. 38: CT sagital image - Same patient as above. Notice that there is no clear fat plane between the mass and the ipsilateral diaphragmatic leaflet, which shows some degree of thickening in its anterior portion.
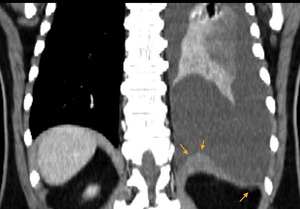
Fig. 39: Thorax CT coronal image - 52 year-old female with metastatic melanoma. There is thickening of the left diaphragmatic leaflet and there are metastatic implants in the abdominal surface.

Fig. 40: CT axial image - Same patient as above. This image better depicts the metastatic implants, both in the thoracic and abdominal surfaces of the left hemidiaphragm.

Fig. 41
Diaphragmatic tears are uncommon and usually occur secondarily to high impact,
being associated with other severe injuries,
such as splenic and renal trauma,
in 81% of cases.
Diaphragmatic tears are more frequent on the left, due to presence of the liver on the right.
Nevertheless,
delayed presentation of tears on the right can lead to life threatning conditions such as bowel herniation and strangulation.
On chest radiography,
specific findings of diaphragmatic tear include intrathoracic hollow viscus herniation at the site of tear and nasogastric tube above the left hemidiaphragm.
Findings suggestive of rupture include hemidiaphragmatic elevation,
distortion or obliteration of the normal contours.
CT is the modality of choice,
with MPR reformats allowing for high sensitivy and specificity of 78% and 100% in left tears,
and as much as 71% and 100% on right-sided tears.
Some signs of diaphragmatic tear seen with CT are shown on table 2 (Fig.17)

Fig. 42: Thorax CT coronal image - 44 year-old male involved in a high impact vehicle collision. There is a tear on the left hemidiaphragm, and partial herniation of the stomach, which is adjacent to the left ventricle.

Fig. 43: CT axial image - Same patient as above. There is complete loss of the normal contours of the left diaphgram, indicating left tear which was later confirmed at surgery.


