The diaphragm represents the most important muscle involved in the normal ventilation process,
acting also as a physical barrier which separates the thorax from the abdomen.
It can frequently be a cause of dyspnea,
due to dysfunction which can be either intrinsic or extrinsic.

Fig. 5
The diaphragm has multiple attachments to the thoracic wall,
some of which can be seen with CT,
and represents an important landmark for the radiologist.
POSTERIOR ATTACHMENTS
DIAPHRAGMATIC CRURA
They attach the diaphgram to the lumbar vertebral bodies and disks
They are joined by the median arcuate ligament

Fig. 6: CT axial image - 53 year-old patient with metastatic melanoma. This image depicts the normal appearance of the diaphragmatic crura, which can either have a smooth of more nodular appearance.
Notice also the metastatic implants on the left hemidiaphragm.
MEDIAL AND LATERAL ARCUATE LIGAMENTS
Medial: extends over the anterior psoas muscles as fibrous bands between the L1 or L2 vertebral bodies and transverse process of L1
Lateral: fascial bands that cover the quadratus lumborum muscle and extend from the transverse process of D12 to the middle portion of 12th ribs
ANTERIOR AND LATERAL ATTACHMENTS
They include the sternum (xifoid process),
lower six ribs and costal cartilage
These attachments are better depicted with CT
HIATUSES
There are three main hiatuses in the diaphragm which allow the passage of important structures (Fig.2).
1.
The inferior vena cava (IVC) hiatus - This hiatus is localized at the D8 level and contains the IVC and branches of the right phrenic nerve.
It passes through the midportion of the central tendon and enlarges during inspiration.
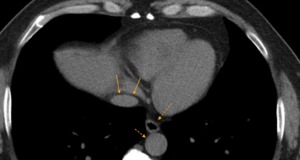
Fig. 7: CT axial image - This image displays the three main diaphragmatic hiatuses, from anterior to posterior: the inferior vena cava hiatus, the esophageal hiatus and the aortic hiatus.
2.
The esophagus hiatus - At the level of D10,
this hiatus (Fig.8) contains the esophagus,
vagus nerve and sympathetic nerve branches.
It passes through the crossing fibers of the right diaphragmatic crus,
which forms a ring around the esophagus and acts like a sphincter,
reducing the occurence of gastroesophageal reflux.
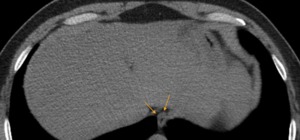
Fig. 8: CT axial image - The esophageal hiatus
3.
The aortic hiatus - This hiatus (Fig.9) lies at D12 level,
containing the aorta,
thoracic duct,
azigos and hemiazigos veins.
It represents the most retrocrural of all hiatuses.

Fig. 9: CT axial image - the aortic hiatus. In this image there is a clear distinction of the diaphragmatic crura and the aorta passing at a posterior level.

Fig. 10
CHEST RADIOGRAPHY
On frontal views (Fig.11),
the dome of the right hemidiaphragm is seen at the level of the anterior sixth rib.
The left dome is usually one intercostal space lower than the right.
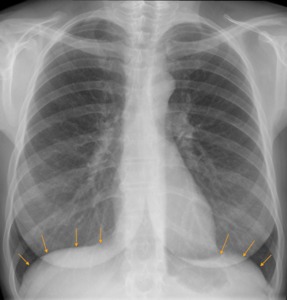
Fig. 11: Chest x-ray PA view. The upper diaphragmatic surface can be easily seen and usually has smooth contours. The right hemidiaphragm can also have a higher position compared to the left, and a difference up to 3cm is still considered normal.
On lateral views,
the anterior part of the left dome is obscured by the cardiac shadow but the right dome is entirely seen.
COMPUTED TOMOGRAPHY
With CT,
the diaphragm is usually seen as a thin sheeth of muscle which separates the thoracic and abdominal cavities.
There are three typical appearances on axial images:
Type 1 (48%) - the central tendon is cephalic to the xiphoid process.
It appears as a ondulating curve of soft tissue,
concave posteriorly and continuous across the midline (Fig.12).
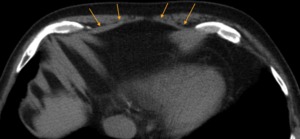
Fig. 12: CT axial slice - Type 1 appearance of the anterior diaphragm.
Type 2 (28%) - the central tendon is caudal to the xiphoid process.
The diaphragm has a discontinuous appearance,
diverging from the midline as it approaches the anterior thoracic wall.
Type 3 (11%) - the central tendon and the xiphoid process are at the same level.
The anterior diaphragm appears as a broad band with irregular and ill defined margins (Fig.13).
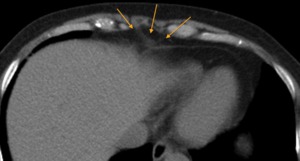
Fig. 13: CT axial image - Type 3 appearance of the anterior diaphragm. Notice that the anterior diaphragm is thick and ill defined, as it runs in the same plane of the image.

Fig. 14
Diaphragmatic innervation is provided by the right and left phrenic nerves (Fig.4) (origin at the C3-C5 level),
which are fundamental for sensory and motor function.
Location: the phrenic nerves are located at the lateral compartment of the neck and travel anteriorly,
coursing through the thorax.
They course through the anterior surface of the pericardium,
before reaching the diaphragm and branching its superior and inferior surfaces.

Fig. 15
The diaphragm is the primary muscle envolved in ventilation.
During inspiration it contracts simultaneously with the acessory ventilatory muscles,
namely intercostal muscles,
sternocleidomastoid and scalene,
and expands the thoracic cavity,
decreasing intrathoracic pressure and allowing entrance of air.
Diaphragmatic dysfunction can be classified as paralysis,
weakness or eventration.
On chest radiography,
it can usually be suggested by elevation of the diaphragm,
either unilateral or bilateral.
It's important to remember that the right dome usually has a higher position than the left dome.




