The male patient presenting with a breast-related complaint is statistically much more likely to be benign in aetiology as fewer than 1% of all patients with breast cancer are men [3]. A noticeable trend is,
however,
that more male patients are being referred for the work up of breast complaints with some breast units reporting an increase of referrals by up to 500% over the last decade or so [4].
Also,
incidental findings on cross-sectional imaging – CT,
MRI and PET-CT scanning constitute an alternative source of a number of asymptomatic lesions for assessment.
Gynaecomastia: the commonest benign condition of the male breast
Males may seek medical attention in the symptomatic breast clinic for such symptoms as breast enlargement,
breast pain or palpable lump.
The majority of breast conditions in the male patient are indeed benign and gynaecomastia is the commonest aetiology.
Gynaecomastia is defined as
an increase in breast size due to a proliferation of breast ducts and stromal tissue secondary to an increased oestrogen to testosterone ratio [5].
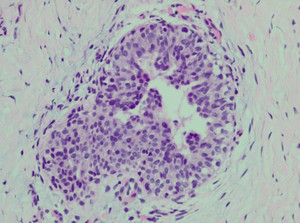
Fig. 1: Histologically, florid gynaecomastia is characterized by intraductal epithelial hyperplasia and increased periductal cellularity and oedema. In the inactive fibrous phase, the epithelial cells are flat and the periductal stroma is hyalinised.
References: Department of Histopathology, Mater Dei Hospital - Birkirkara/MT
Pseudogynaecomastia is defined as a sole increase in the amount of adipose breast tissue.
Gynaecomastia can present at any age but is most commonly seen during puberty and senescence –and hence described as physiologic – with the prevalence of asymptomatic gynaecomastia quoted as being as high as 60-90% in neonates,
up to 60% in adolescence and approaching 70% in men aged 50-69 years [6].
Endocrine and systemic disease,
drugs and some neoplasms are other potential causes of gynaecomastia [5,7].

Table 1: Causes of Gynaecomastia
References: Adapted from: Charlot M, Beatrix O, Chateau, F et al. (2013) Pathologies of the male breast. Diagnostic and Interventional Imaging 94:26‑37
Clinically,
gynaecomastia presents as a soft,
mobile,
tender,
retroareolar mass. It may be a unilateral process (14%). Bilateral symmetrical or bilateral asymmetrical (84%) changes in the breast may be detected clinically [5].
The main differential for gynaecomastia is lipomastia or pseudogynaecomastia which is the deposition of increased adipose tissue subcutaneously.


 Pathologies of the male breast. Diagnostic and Interventional Imaging 94:26‑37")