Paraduodenal or Groove Pancreatitis (GP) is an uncommon type of focal chronic pancreatitis affecting the groove between the head of the pancreas,
the duodenum,
and the common bile duct.
GP can be subdivided into a pure form which affects exclusively the groove,
sparing the pancreatic head (Figure 1 A),
and a segmental form,
which also extends to the pancreatic head with a clear predominance in the groove (Figure 1 B).
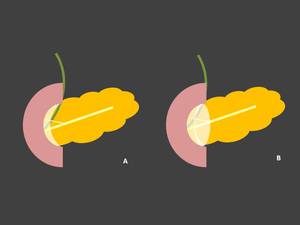
Fig. 1: Illustrations of groove pancreatitis. (A) Represents pure form of GP with fibrotic tissue only in pancreaticoduodenal groove. (B) Drawing depict fibrotic tissue in pancreaticoduodenal groove also involving pancreatic head, segmental form of GP.
Findings of groove pancreatitis associated to diffuse chronic pancreatic disease should be included in GP,
because a pure or segmental form can cause progressive stenosis of the pancreatic duct and consequently lead to diffuse chronic pancreatitis.
Patients affected by GP are relatively young men with a history of alcohol abuse in the majority of cases.
The disease has been sporadically described in women.
The reason for male predilection in GP is still unknown.
The pathogenesis of GP also remains unclear,
although several factors may be implicated,
including previous diseases of the biliary system,
peptic ulcer,
gastric hypersecretion,
gastric resection,
true duodenal wall cyst,
pancreatic heterotopia in the duodenum or disturbance of the flow of pancreatic juice through the Santorini duct.
The typical location of the lesions around the minor papilla suggests the presence of an anatomical or functional predisposing condition at this region.
A significant number of patients with GP have absent or a narrow Santorini duct or pancreas divisum: the resistance caused by the accessory outflow through the Santorini duct may render pancreatic tissue vulnerable to alcohol injury.
In addition,
pancreatic heterotopias with the presence of pancreatic tissue at the duodenal wall is seen in some cases of GP,
indicating the incomplete involution of the dorsal pancreas at this region,
functioning as a predisposing factor for this disease.
The histopathologic hallmark of GP is the presence of fibrotic tissue in the pancreaticoduodenal groove only or in the groove and the superior portion of the pancreatic head,
in the pure and segmental forms of the disease,
respectively.
The duodenum is always wrapped by a chronic inflammatory process,
with fibrotic tissue and different levels of stenosis.
Hyperplasia of Brunner’s glands is seen in most of the cases.
Cystic lesions,
either true cysts or pseudocysts,
are common in the groove or the duodenal wall,
and they are believed to represent cystic dystrophy of a heterotopic pancreas in the duodenal wall.
The clinical presentation of GP is related primarily to duodenal and biliary obstruction.
It is similar to the usual form of chronic pancreatitis,
but recurrent vomiting,
attributable to marked duodenal stenosis and impaired motility,
tends to be more pronounced in GP.
Jaundice is unusual,
and when present,
often fluctuates,
in contrast to the continuously progressive jaundice found in patients with pancreatic carcinoma.
Weight loss can also be encountered,
further complicating the differential diagnosis with pancreatic cancer.
The duration of clinical symptoms ranges from a few weeks to more than 1 year,
with most patients presenting symptoms from 3 to 6 months.
Acute presentation of gastric outflow obstruction may also occur in a minority of cases.
Blood tests often show a slight elevation of serum pancreatic enzymes,
such as amylase,
and occasionally of serum hepatic enzymes.
Bilirubin elevation is also detected in patients who are clinically jaundiced at presentation.
Patients with chronic symptoms may develop exocrine pancreatic insufficiency or diabetes.
The differential diagnosis of the pure form of GP includes duodenal cancer,
cholangiocarcinoma or acute pancreatitis with phlegmon along the groove.
MRCP is useful for differentiating GP from common biliary duct (CBD) cancer,
since the former shows a long segmental smooth CBD stenosis or tapering.
The signal characteristics of the sheetlike mass on MR images in GP are useful for differentiation from acute pancreatitis,
where the phlegmon exhibits high signal intensity on T2-weighted images.
Differential diagnosis should also include chronic pancreatitis in acute transformation with pseudocysts in the duodenal wall that differs from GP because of the absence of duodenal wall thickening or stenosis,
and of true cysts in the duodenal wall or in the groove area which are typical in GP.
In cases of the segmental form of GP when a pancreatic mass is evident,
the differential diagnosis from pancreatic adenocarcinoma is challenging.
An important differentiating clue is the normal appearance of the peripancreatic vessels in GP that may be displaced,
but they do not show signs of obstruction or encasement.
In contrast,
pancreatic adenocarcinoma apparently extending to the peripancreatic tissue or the duodenum with invasion along large peripancreatic vessels that are obstructed or encased.
The typical location of GP is an important key finding for the radiological differentiation from pancreatic carcinoma.
Yet the distinction between fibrous tissue in GP and scirrhous adenocarcinoma of the pancreatic head invading the groove is difficult on MR imaging.
Both lesions can present duodenal wall thickening and lumen narrowing,
show hypointensity on T1-weighted images and may also exhibit delayed enhancement at the late phase on dynamic study.
Differential diagnostic clues are the absence of duodenal cystic lesions; abrupt,
circumscribed,
irregular stenosis or complete ductal obstruction of the intrapancreatic portion of the bile duct; and the frequent sparing of the main pancreatic duct in most cases of groove adenocarcinoma.
Duodenal biopsies may contribute to the correct diagnosis,
but still,
if the pancreatic carcinoma in the groove area is small and does not invade duodenal mucosa,
the distinction between inflammatory mass and carcinoma may be quite difficult.
In any case the presence of GP does not exclude the development of a pancreatic adenocarcinoma.
In those situations the marked pancreatic duct dilatation,
more than expected in the segmental form of GP,
even in the presence of a sheet-like mass in the groove area,
should be suspicious for the presence of adenocarcinoma.
