1.
EPIDEMIOLOGY:
1.1.
Data from an injury surveillance study conducted during the 2006-2007 triathlon race season in Victoria,
Australia. Source: Gosling CM,
et al.
Am J Sports Med 2010; 38:1007-14
Of 10,197 individual starters who took part:
- 217 triathletes on a total of 235 occasions sought medical assistance (n = 322 injuries)
- 2.3% of the total race starters
- 20.1 injury presentations per 1000 hours of competition
- Injuries sustained mostly during the run (38.4%) and cycle (14.3%) legs
- Lower limb injuries (59.5%) = most common site of injury
- Abrasions (28.6%) = most common nature of injury
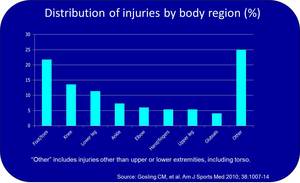
Fig. 1: Distribution of injuries by body region.
References: Gosling CM, et al. Am J Sports Med 2010; 38:1007-14
1.2.
Data from 2011 Norseman Xtreme Triathlon (Source: Clarsen B,
et al.
Br J Sports Med 2013; 47:495-502 & Andersen CA,
et al.
Br J Sports Med 2013; 47:857-61)
- 174 participants filled out Oslo Sports Trauma Research Center Overuse Injury Questionnaire during their training period before the competition
- 26-week prospective data collection period leading up to the day of competition
- Average weekly prevalence of symptoms related to overuse injuries (e.g.
pain,
ache,
swelling,
stiffness,
looseness):
- Shoulder 20%
- Thigh 12%
- Knee 25%
- Lower leg 23%
2.
SHOULDER INJURIES:
The majority of triathletes use the freestyle stroke during swimming.
- Repetitive abduction,
flexion and extension motion against resistance may result in overuse injuries (e.g.
rotator cuff tendinopathy,
bursopathy,
shoulder impingement).
- The biceps tendon and rotator cuff must pass rapidly under the coracoacromial arch.
- The supraspinatous and biceps tendons are most commonly affected by tendinopathy.
Swimmer’s shoulder
- a combination of rotator cuff tendinitis,
impingement and laxity,
due to overstretching of the anterior glenohumeral ligament.
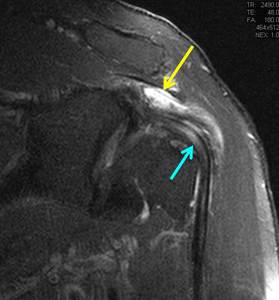
Fig. 2: 34-year-old male triathlete. Coronal PD-w fat suppressed image shows subacromial bursitis (yellow arrow) and biceps tendinopathy(blue arrow).
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
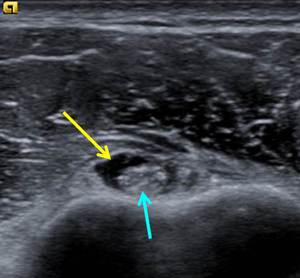
Fig. 3: 29-year-old male triathlete. Ultrasound shows biceps tenosynovitis after strenuous swimming training. Note the hypoechoic fluid (yellow arrow) surrounding the abnormally echogenic biceps tendon in the bicipital groove and biceps tendinopathy (blue arrow).
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
Acromioclavicular osteoarthritis
- May occur due to overuse or secondary to previous acute trauma to the acromioclavicular joint and may result in chronic shoulder pain.
- Osteolysis of the distal clavicle may be seen as a complication.
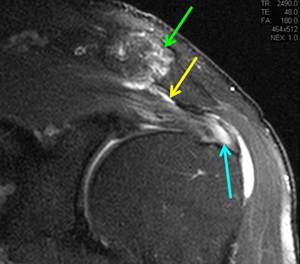
Fig. 4: 51-year-old male triathlete. Coronal PD-w fat suppressed image shows AC joint arthritis (green arrow), subacromial bursitis (yellow arrow) and advanced supraspinatus tendinosis (blue arrow).
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
Paget-Schroetter syndrome
- AKA effort thrombosis.
- Subtype of venous thoracic outlet syndrome,
usually as a result of overhead arm physical activity and can be seen in triathletes.
- Compression of subclavian vein at the costoclavicular junction,
with resultant venous damage and eventually venous thrombosis.

Fig. 5: 37-year-old male triathlete. Venogram (LEFT) shows acute stenosis at the junction of the left axillary and left subclavian veins at the level of the first rib (arrow). Coronal MR venogram (RIGHT) confirming an acute stenosis at the junction of the left axillary and subclavian veins (arrow). No external cause could be identified in this case.
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
3.
ELBOW AND WRIST INJURIES:
- The use of traditional handle bars during cycling results in compressive forces on the wrist in an extended position.
- May result in ulnar nerve compression and a condition similar to carpal tunnel syndrome.
- Motor and sensory deficits are more common in the ulnar nerve distribution.
De Quervains tenosynovitis
- Most common tendinopathy of the wrist in athletes.
- Caused by a shearing stress injury of the first extensor compartment tendons along the radial styloid.
- Repetitive wrist motion with radial or ulnar deviation and flexion or extension may result in tenosynovitis or even tearing of the extensor pollicis brevis and abductor pollicis longus tendons.
Intersection syndrome
- Overuse injury as a result of repetitive microtrauma.
- AKA oarsmen’s wrist,
squeaker’s wrist or crossover syndrome.
- MRI shows peritendinous edema concentrically surrounding the 1st and 2nd extensor compartment tendons (abductor pollicis longus and extensor pollicis brevis) around the point of crossover ~ 4 cm proximal to the Lister tubercle.
- Edema may extend as far distally as the radiocarpal joint.
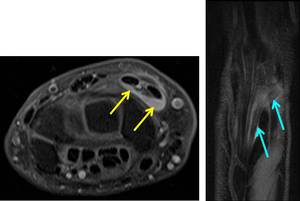
Fig. 6: (LEFT) Axial PD-w FS image in a 35-year- old female elite triathlete shows fluid (yellow arrow) surrounding the extensor carpi radialis (ECR) longus and brevis tendons, where the abductor pollicis longus (APL) and extensor pollicis cross the ECR tendons. This was thought to be secondary to the use of her triathlon bars for extended periods of time. (RIGHT) Coronal oblique PD-w FS image showing the “crossing over” of the APL over the ECR tendons (blue arrow).
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
4.
HIP INJURIES:
Hip injuries are mostly associated with running,
although cycling may also account for or exacerbate a number of conditions.
Three bursal groups are found about the hip.
- Trochanteric,
ischiogluteal and iliopsoas bursae.
The trochanteric bursa consists of:
- subgluteus maximus bursa
- subgluteus medius bursa
- subgluteus minimus bursa
Hip bursopathy (greater trochanter pain syndrome)
- Often associated with gluteus medius and minimus tendinopathy.
- More commonly seen in women,
likely because of the wider pelvis.
- Running on a cambered road,
an unusually prominent trochanter and runners with excessive adduction are further risk factors.
- MRI demonstrates distention of the bursae with fluid.
- Signs of inflammation and/or hemorrhage include synovial thickening,
internal debris,
septations,
and fluid-fluid levels.
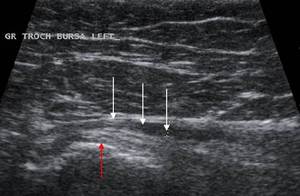
Fig. 7: Ultrasound image shows a chronically distended trochanteric bursa (white arrows) in a 54 year-old female triathlete training for a long distance triathlon. Note the intact gluteus medius tendon inserting onto the greater trochanter (red arrow).
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
Snapping hip syndrome
- AKA coxa saltans,
iliopsoas tendinopathy or dancer’s hip.
- Presents as an often painful snapping sensation and/or audible snapping sound that occurs at the hip during a specific motion.
- More common amongst younger athletes.
External snapping hip syndrome
- caused by either the iliotibial band,
tensor fascia lata or tendon of the gluteus maximus muscle rapidly sliding over the greater trochanter.
- is often a clinical diagnosis and rarely requires imaging.
Internal snapping hip syndrome
- is more complex and may occur when the iliopsoas tendon slides over the iliopectineal eminence,
femoral head,
lesser trochanter or the anterior hip capsule.
- may also occur when the biceps femoris tendon slides over the ischial tuberosity or the iliofemoral ligament slides over the femoral head.
- Ultrasound is the investigation of choice for dynamic evaluation of the iliopsoas tendon in internal snapping: seen as a sudden lateral-to-medial movement of the tendon as it passes over the iliopectineal eminence.
- Ultrasound can also be used for image guided injection of a combination of a local anaesthetic and a corticosteroid into the iliopsoas bursa.
- Further causes of internal snapping include labral tears,
intra-articular loose bodies,
synovial osteochondromatosis and fracture fragments: can be effectively evaluated by MR arthrography.
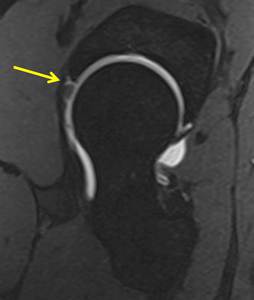
Fig. 8: Sagittal DESS post-arthrographic study shows contrast intravasation into a tear of the anterosuperior labrum (arrow) in an elite 29-year-oldmale triathlete.
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
Piriformis syndrome
- Isolated sciatic pain affecting the buttock with radiation to the upper thigh,
but without sensory fallout.
- Described radiological features include piriformis muscle hypertrophy and an anomalous course of the S2 nerve root,
most notably an intramuscular course traversing through the piriformis muscle.
- Absence of more common causes of sciatica such as lumbar disc herniation.
- Image-guided injection of the piriformis muscle initially with air (marker) followed by local anesthetic and cortisone can be used as a diagnostic test.
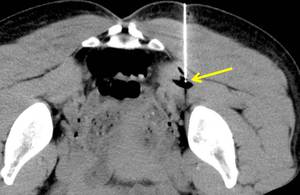
Fig. 9: CT-guided infiltration. Axial prone CT image of the pelvis demonstrates asymmetric enlargement of the left piriformis muscle in a 40-year old female triathlete with left-sided radiculopathy. Percutaneous needle placement was performed under CT guidance with the tip visible in the piriformis muscle belly (arrow). Air was instilled, visible at the needle tip and dissecting along the intramuscular planes. The patient experienced rapid improvement of symptoms and remains asymptomatic.
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
Osteitis pubis
- Part of the entity known as athletic pubalgia.
- Occurs as a result of repetitive vertical shearing forces across the pubic symphysis.
- MRI demonstrates bone marrow edema at the pubic symphysis.
- May be associated with adductor tendinopathy,
posterior abdominal wall weakness and incipient inguinal hernia (Gillmore’s groin).
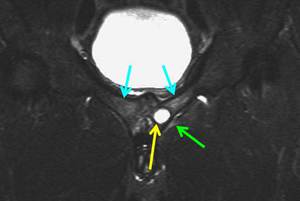
Fig. 10: 30-year-old triathlete with chronic groin pain, most severe with running. Coronal STIR image of the pelvis shows bilateral bone edema of the pubic bones (blue arrow) and an intraosseous cyst in the left body of the pubis (yellow arrow). Hyperintense signal is also present at the insertion of the left adductor muscle group (green arrow), representing edema as a manifestation of insertional enthesopathy, which form a part of the condition known as athletic pubalgia.
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
5.
THIGH INJURIES:
Morel-Lavallée lesion
- Commonly seen in off-road triathlons due to falls off the mountain-bike.
- Closed degloving soft tissue injury as a result of shearing forces during blunt trauma. A potential space is created between the subcutaneous tissue and superficial fascial layer,
which fills up with blood products,
lymph and necrotic fat,
creating a mass-like subcutaneous fluid collection.
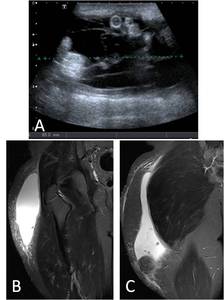
Fig. 11: 18-year-old male triathlete presented with a large swelling of the right proximal thigh following a fall during a competition. Ultrasound image (A) demonstrates the presence of a large fluid collection. Coronal T2-w fs images (B and C) show a large subcutaneous seroma in the right thigh, consistent with Morel-Lavallée lesion.
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
6.
KNEE INJURIES:
Knee injuries are most commonly caused by excessive running and exacerbated by running and cycling.

Fig. 12: Sagittal PD-w image shows a horizontal flap tear of the posterior horn of the medial meniscus.
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
Common overuse injuries:
- Patellar tendinopathy
- Patellofemoral stress syndrome
- Iliotibial band friction syndrome (ITBS)
Patellar tendinopathy (“Jumper’s knee”)
- = Tendinopathy at the proximal enthesis
- Acute anterior knee pain during running and cycling.
- During cycling,
the high extension forces during the down stroke places strain on the patellar tendon (e.g.
hill climbing and cycling whilst standing).
- Ultrasound is initial imaging modality: hypoechoic focus in the tendon; associated increased echogenicity in the adjacent Hoffa fat pad; abnormal focus of tendinosis may demonstrate increased Doppler signal (neovascularization).
- MRI reveals thickening of the tendon with increased signal intensity on fluid-sensitive sequences. Bone marrow edema may be present in the inferior pole of the patella.

Fig. 13: Sagittal PD-w fs image of the knee with thickening and increased signal intensity in the proximal patellar tendon. There is associated bone marrow edema of the inferior patellar pole with soft tissue edema present in Hoffa’s fat pad. Features represent infrapatellar tendinosis.
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
Patellofemoral stress syndrome
- Also called “runners knee” or “bikers knee”.
- Causes are multifactorial: Overuse,
trauma and abnormal biomechanics; Quadriceps muscle imbalance with relative deficiency of vastus medialis obliquus muscle group.
- More common in female triathletes.
- X-rays may be normal or may demonstrate a patella alta,
lateral subluxation of the patella and/or features of trochlear dysplasia.
- MRI is the investigation of choice to assess the patellofemoral chondral surfaces. Chondral degeneration,
delamination,
chondral defects with a bone stress reaction and eventually patellofemoral osteoarthrtis may occur.
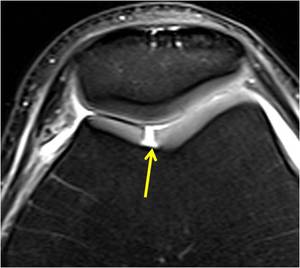
Fig. 14: Axial PD-w fs image shows a full-thickness cartilage defect of the femoral trochlea (arrow).
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
Iliotibial band friction syndrome
- Due to repetitive friction between the distal iliotibial band and the lateral femoral condyle.
- Manifests as lateral knee pain.
- Usually occurs between 10 – 30o of knee flexion.
- Running and cycling may result in and cause aggravation of this condition.
- Factors that may increase the risk: The seat is too high or too far back during cycling; Running on cambered road,
downhill running treadmill running; Leg length discrepancy; Rapidly increasing weekly running; Weak hip abductors.
- MRI findings include poorly defined high signal intensity or a circumscribed fluid collection deep to the iliotibial band on fluid-sensitive sequences.
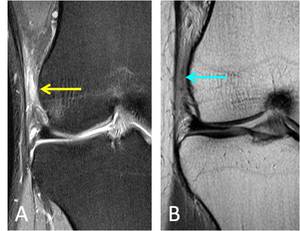
Fig. 15: A. Coronal PD-w fs image of the knee with hyperintense signal and fat stranding deep to the iliotibial fascial band and superficial to the lateral femoral epicondyle (yellow arrow).
B. Coronal PD-w image confirms hypointense signal (blue arrow) deep to the iliotibial fascial band, in keeping with iliotibial band friction syndrome.
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
Plica syndrome
- Painful impairment of knee function with a thickened and fibrotic plica.
- Thought to be secondary to the hyperflection position of the knee during extended periods in the aero position (= lying with the torso on handle bars).
- May be associated with effusion/synovitis.
- May also result in erosion of the femoral condyle and/or patellar cartilage damage.
- Commonly affected plicae include the infrapatellar,
suprapatellar and mediopatellar plicae (=most common).

Fig. 16: Elite triathlete presented with anterior knee pain thought to be secondary to long hours in the aero position during cycling, clinically thought to be due to a symptomatic plica (arrow). Axial PD-w fs (A) and axial PD-w images (B) show a thickened, hemorrhagic plica projecting into the patellofemoral joint. Arthroscopic image (C) shows a thickened, hemorrhagic plica.
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
Popliteal artery entrapment syndrome
- = Vascular compression syndrome.
- Characterized by compression of the popliteal artery between the two heads of the gastrocnemius muscle.
- Compression may result in thrombosis with or without distal embolization as well as aneurysm formation.
- The underlying etiology is anatomic variation in the relationship between the gastrocnemius muscle and the popliteal artery.

Fig. 17: Axial PD-w image shows an anomalous origin of the medial gastrocnemius muscle (arrow), which can result in popliteal artery compression syndrome.
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
Cystic adventitial disease
- Characterized by luminal compression 2o to mucoid cysts formation in the adventitia.
- Rapidly progressive calf claudication.
- Typically affects men between 20 and 50 years without atherosclerotic risk factors.
- Popliteal arteries most commonly affected.
- Repetitive adventitial microtrauma may be an etiological factor. May occur in conjunction with popliteal artery entrapment syndrome.
- Ultrasound and MRI may demonstrate focal cystic lesions in the adventitia with associated luminal narrowing.
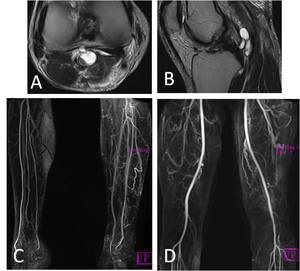
Fig. 18: 37-year-old male triathlete presented with chronic symptoms of calf claudication during the running leg. (A) Axial PD-w image shows a cyst-like lesion related to the popliteal artery. (B) Sagittal T2-w image confirms a cyst-like lesion related to the popliteal artery. (C) MRA shows significant collateral arterial formation in the left calf. Normal arterial anatomy on the right. (D) MRA shows left popliteal artery stenosis, with arterial collaterals proximal and distal to the stenosis.
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
Stress fracture
- Osseous stress injuries occur when the normal adaptive response of osteoclastic bone resorption and osteoblastic bone formation is unable to keep up with the increased loading and microtrauma.
- Stress fractures are most common along the weight-bearing axis of a bone; Medial cortices of long bones more commonly affected; Medial proximal tibia most commonly affected.
- Gradual onset pain,
worse on weight-bearing.
- MRI demonstrates bone marrow edema on fluid-sensitive sequences.
- A fracture line may be seen on T1-w and PD-w images.
- Some sites are more prone to non-union; Anterior tibia,
medial malleolus,
talus,
navicular,
fifth metatarsal and first metatarsal sesamoids.
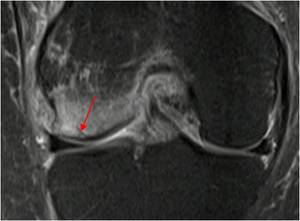
Fig. 19: Middle-aged female triathlete presented with insidious onset knee pain, thought to be a meniscal tear. MR shows a subchondral fatigue fracture (arrow) with extensive surrounding bone marrow edema. The menisci were intact.
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
7.
CALF INJURIES:
Medial tibial stress syndrome (MTSS)
- Commonly known as shin splints.
- Characterized by tenderness along the posteromedial aspect of distal third of tibia.
- More common in women.
- Is a spectrum of overuse injury including periostitis,
bone stress reaction and/or repetitive traction tendinopathy of the tibialis posterior tendon.
- MRI features include a linear area of high signal intensity along the posteromedial border of the tibia on fluid-sensitive sequences.
- Important to distinguish MTSS from tibial or fibular stress fractures and compartment synd.
- MRI demonstrates cortical abnormalities such as cortical resorption cavities present in stress fractures but not in MTSS.
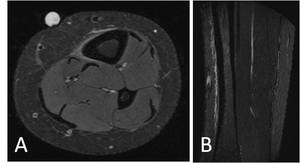
Fig. 20: A. Axial STIR image of the proximal tibia in a triathlete presenting with anterior tibial pain whilst running. An oil marker was placed on the skin at the point of maximal tenderness. Periosteal thickening and edema is present on the anteromedial aspect of the tibia.
B. Sagittal STIR image of the same patient with linear periosteal thickening and edema present along the anterior tibia, consistent with a medial tibial stress syndrome. Note the absence of bone marrow edema in both images.
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
Delayed onset muscle soreness (DOMS)
- Characterized by painful muscle stiffness usually resulting from an unfamiliar exercise,
especially during eccentric exercise such as running downhill,
or exercise of unusual intensity or duration.
- Pain,
stiffness and swelling as well as loss of stiffness and loss of coordination can occur,
usually affecting a defined muscle group.
- Symptoms tend to peak at 48 hours after which it improves spontaneously over 3 to 10 days.
- The role of MRI is controversial.
However,
persistent soft tissue edema of the affected muscle group could aid in confirming the diagnosis.
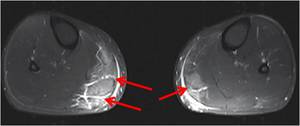
Fig. 21: Amateur triathlete presented with severe pain while walking two days after a middle-distance triathlon. Axial PD fs image of the lower legs shows increased signal in and around the medial gastrocnemius muscles (arrow), more severe on the right. Features are compatible with delayed onset of muscle soreness.
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
8.
ANKLE INJURIES:
Achilles tendinopathy
- Due to repetitive plantar flexion against resistance,
as occurring on the down stroke during cycling.
- More common amongst older athletes.
- Exacerbated by having to cycle immediately after the ankle has been in prolonged plantar flexion during the swimming leg.
- May be due to the use of racing shoes or minimalistic running shoes that have a lower heel than standard running shoes.
- Two types of tendinopathies:
- Hypoxic type presents with a painless lump. MRI demonstrates a focal area of thickening with low signal intensity on T1- and T2-w imaging.
Normal echogenicity is noted on ultrasound. This type is associated with a small risk of progression to rupture.
- Mucoid type presents with focal painful thickening.
Fluid-sensitive sequences demonstrate linear hyperintensity whilst on ultrasound linear hypo- to anechoic areas can be seen. This type has a high likelihood of progression to rupture if not managed correctly.
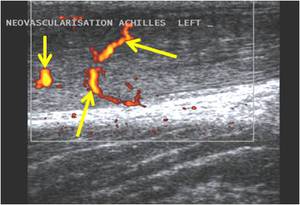
Fig. 22: Ultrasound image of Achilles tendinosis with neovascularization in an amateur middle-aged triathlete who switched to minimalistic running shoes without proper periodization. Arrows point to neo-vessels with the tendon.
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
Sural nerve entrapment
- The sural nerve: is entirely sensory; courses along the posterolateral aspect of the distal calf in close association with the short saphenous vein; terminates in the lateral dorsal cutaneous nerve and the lateral calcaneal branches.
- Entrapment of the nerve usually occurs proximally.
- It may be as a result of direct compression of the adjacent short saphenous vein or due to trauma with ensuing fibrosis,
resulting in symptoms similar to neuropathy.
- MRI is the investigation of choice.
- Imaging may reveal a causative compressive lesion,
perineural fibrosis or a focal neuroma similar to a Morton’s neuroma or it may be normal.

Fig. 23: Coronal PD-w image demonstrates extensive fat stranding and linear hypointense fibrotic changes in the posterior soft tissues of the ankle surrounding the sural nerve, resulting in entrapment of the nerve and severe pain in the sural nerve distribution.
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
9.
FOOT INJURIES:
Metatarsalgia
- Clinical entity of pain over the metatarsal heads.
- It encompasses a large amount of etiologies including tendinitis,
metatarsophalangeal joint synovitis / capsulitis,
metatarsal stress reaction,
metatarsal stress fractures,
sesamoiditis and Morton’s neuroma.
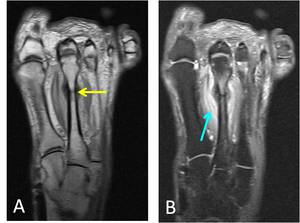
Fig. 24: A. Long axis T1-w image of the foot shows a healing stress fracture of the shaft of the 2nd metatarsal (yellow arrow). Note the exuberant callus formation.
B. Long axis STIR image of the foot in the same patient also demonstrates persistent surrounding soft tissue edema (blue arrow).
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
Plantar fasciitis
- Plantar fascia extends from the medial calcaneal tubercle to the metatarsal heads (= supportive longitudinal arch).
- Overuse or stretch injury results in tendinopathy or partial tearing of the medial plantar aponeurosis.
- Cycling may exacerbate the condition.
- Represents 50% of running foot and ankle injuries.
- Ultrasound demonstrates a thickened aponeurosis of more than 5mm as well as increased Doppler flow.
- MRI demonstrates increased signal intensity within and around a thickened medial plantar aponeurosis on fluid-sensitive sequences. It is often associated with bone marrow edema of the calcaneus.
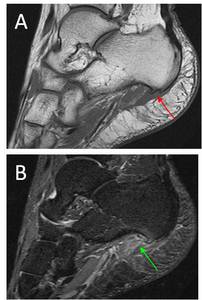
Fig. 25: A. Sagittal PD-w image of the hindfoot demonstrates a plantar calcaneal spur (red arrow). There is associated thickening and increased signal intensity of the plantar fascia at the insertion.
B. Sagittal STIR image of the hindfoot demonstrates increased signal intensity of the plantar fascia at the insertion (green arrow). There is also surrounding soft tissue edema. These findings are consistent with plantar fasciitis.
References: Department of Radiology, Boston University School of Medicine and Van Wageningen and Partners
