ECR 2015 / C-0288
Radiological findings in patients with Crouzon syndrome
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2015
Poster Number:
C-0288
Type:
Educational Exhibit
Keywords:
Pathology, Genetic defects, Epidemiology, Education, Diagnostic procedure, MR, CT, Conventional radiography, Paediatric, Neuroradiology brain, Head and neck
Authors:
Z. Grodzicka; Olsztyn/PL
DOI:
10.1594/ecr2015/C-0288

Fig. 1:
The top view of human skull showing cranial sutures.

Fig. 2:
Brachycephaly caused by premature fusion of coronal sutures.

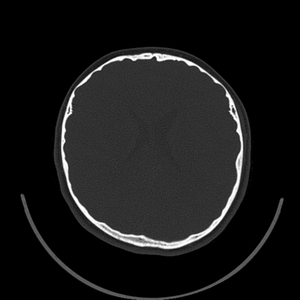
Fig. 3:
CT, axial view of skull showing brachycephaly.

Fig. 4:
CT, axial view of skull showing brachycephaly.

Fig. 5:
Brachycephaly in 18-year-old patient with Crouzon syndrome.

Fig. 6:
Brachycephaly in 18-year-old patient with Crouzon syndrome.

Fig. 7:
Oxycephaly caused by premature fusion of coronal and sagittal sutures.

Fig. 8:
Oxecephaly in 8-year old patient with Crouzon syndrome.

Fig. 9:
Oxecephaly in 8-year old patient with Crouzon syndrome.

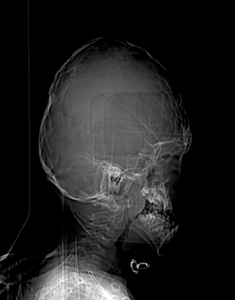
Fig. 10:
Radiograph showing oxycephaly.

Fig. 11:
Radiograph showing oxycephaly.

Fig. 12:
11-year-old girl with Crouzon syndrome.

Fig. 13:
11-year-old girl with Crouzon syndrome.
")
Fig. 14:
younger sister of the girl from Fig.13 (also diagnosed with Crouzon syndrome)
")
Fig. 15:
Father of these two girls (not diagnosed with Crozuon syndrome)

Fig. 16:
Radiograph showing midface hypoplasia.

Fig. 17:
Hypoplasic maxilla with small dental arch.

Fig. 18:
Hypoplasic maxilla with small dental arch.

Fig. 19:
CT, axial view showing hyperthelorism

Fig. 20:
10-year-old girl with Crouzon syndrome, low-set ear.

Fig. 21:
MRI axial plane, distortion of the brain caused by skull deformity.

Fig. 22:
MRI axial plane, distortion of the brain caused by skull deformity.

Fig. 23:
MRI sagittal plane, distortion of the brain caused by skull deformity.

Fig. 24:
MRI sagittal plane, small crowded posterior fossa.

Fig. 25:
MRI axial plane, ventriculomegaly.

Fig. 26:
MRI coronal plane, ventriculomegaly.

Fig. 27:
MRI sagittal plane, ventriculomegaly with cerebral shunt in right lateral...

Fig. 28:
MRI sagittal plane, herniation of the cerebellar tonsils in Chiari I...

Fig. 29:
MRI sagittal plane, Chiari I malformation and syryngomyelia.

Fig. 30:
MRI sagittal plane hypoplasia of corpus callosum, absence of septum pellucidum...

Fig. 31:
MRI coronal plane, hypoplasia of corpus callosum, absence of septum pellucidum...

Fig. 32:
MRI axial plane, hypoplasia of corpus callosum, absence of septum pellucidum...

Fig. 33:
MRI, emissary veins going through foramen cecum draining venous blood from...