All the patients (n=72) with bilateral SNHL underwent HRCT (16-slice) & high-field MRI (1.5T).
The age range of study population varied between 6 months to 20 years.
HRCT of temporal bone aws performed with the following parameters:
1.
0.75-mm collimation,
0.625-mm section thickness,
140 kVp,
120 mAs,
pitch of 0.8,
a 15-cm field of view,
and a 512 x 512 matrix.
The initial data sets were then reconstructed at 0.1-mm intervals.
MR scanning was performed with following sequences.
1.
3D FIESTA(Fast Imaging Employing Steady-state Acquisition) was performed with these parameters: 10-cm FOV,
TR/TE of 8/4,
32 sections of 1-mm thickness,
256 x 256 matrix,
flip angle of 45°,
bandwidth of ± 32 kHz,
two phase cycles,
and an acquisition time of 2 minutes 24 seconds.
Phase-cycling involved two 3D steady-state datasets acquired sequentially,
each with a specific radiofrequency phase shift added at every TR.
2.
For better image resolution of nerves oblique parasagittal view which was perpendicular to the plane of the internal auditory canal (IAC) is taken on both sides.
The cochlea can be further evaluated by generating MIP images.
The process is the same as that used in MR angiography,
except the inner ear is targeted in the reformatting process.
3.
For screening of brain T2W (TE 102.9ms,
TR 4780ms) sequence in Axial plane is taken.
EMBRYOLOGY OF INNER EAR: Fig. 1
At approximately the third week of gestation,
otic placodes arise from the surface ectoderm on each side of the rhombencephalon.
The otic placodes subsequently invaginate and form otocysts,
which are the otic and auditory vesicles.
At around the fifth week,
diverticulum buds from the otocysts form the endolymphatic sacs,
followed by the cochlea and vestibules.
The membranous cochlea achieves 1 to 1 ½ turns at the end of 6 weeks,
and 2 ½ turns are formed at the end of the 7th week.
The semicircular canals start to develop from the utricle segments of the otocysts at 7–8 gestational weeks.
The superior canals form first,
followed by the posterior and then the lateral canals.
The inner ear structures have an adult configuration by the end of 8 weeks (3).
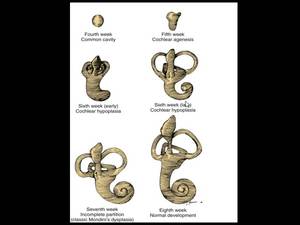
Fig. 1: Image showing process of embryogenesis of inner ear from 4th week to 8th week of gestation.
References: Jackler RK et al, (1987) Congenital malformations of the inner ear: a classification based on organogenesis. Laryngoscope 97:2–14.
Ossification begins in the cochlea,
followed by the semi-circular canals.
Apposition of a shell of ossification proceeds rapidly between 18 and 24 weeks of gestation.
There is very little subsequent remodelling after birth.
The internal auditory canal,
vestibular aqueduct,
mastoid,
and external auditory canal continue to grow after birth (3).
RADIOLOGICAL ANATOMY OF INNER EAR
Fig. 2
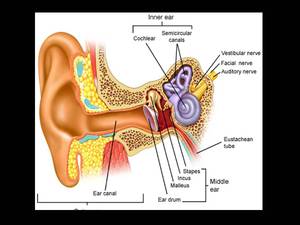
Fig. 2: Image showing anatomy of middle and inner ear
References: Saladin KS. (2004) Anatomy and physiology- the unity of form and function. 3rd ed. New York: McGraw-Hill;
Bony Labyrinth The bony labyrinth consists of the vestibule,
semicircular canals and cochlea
Vestibule
The central portion of the cavity of the bony labyrinth is the vestibule.
The vestibule is a relatively large ovoid perilymphatic space measuring approximately 4 mm in diameter.
The vestibule is continuous anteriorly with the cochlea and posteriorly with the semicircular canals.
There are cribrose areas,
minute openings for the entrance of the nerve branches from the vestibular nerve on the medial wall and floor of the vestibule,
where the vestibule abuts the lateral end of the internal acoustic canal.
The vestibule has two other openings,
the oval window (for the footplate of the stapes) and the vestibular aqueduct.
Semicircular Canals
The three semicircular canals are continuous with the vestibule.
Each of the canals makes about two thirds of a circle and measures about 1 mm in cross-sectional diameter.
Each canal is enlarged anteriorly by an ampulla.
The nonampulated ends of the superior and posterior semicircular canals join to form the bony common crus.
The perilymphatic space of each semicircular canal opens into and communicates freely with the vestibule at both ends.
Cochlea
The cochlea is a conical structure,
its base facing the internal auditory canal and its apex or cupola directed anteriorly,
laterally,
and slightly downward.
The base measures around 9 mm,
and its axis height is about 5 mm.
The base is perforated by numerous apertures for the passage of the cochlear nerve.
The cochlea consists of a bony canal wound around a conical central core called the modiolus.
The modiolus is the conical central pillar of the cochlea.
Its base is broad and appears at the lateral end of the internal acoustic canal,
where it corresponds with the cochlear exit of the corresponding part of the eighth cranial nerve.
It is perforated by numerous orifices for the transmission of the branches of the nerve.
The bony cochlear canal takes between 2 ½ and 2 ¾ turns around the modiolus.
The first turn bulges toward the tympanic cavity,
and this elevation on the medial wall of the tympanic cavity is known as the promontory.
The cross-sectional diameter of the beginning of the canal is about 3 mm.
The openings in or near the first portion of the cochlear canal include the round window,
which is covered by the secondary tympanic membrane; the oval window (actually an opening of the vestibule),
which is covered by the footplate of the stapes; and the cochlear canaliculus,
which leads via a small canal to the subarachnoid s The bone separating one turn of the cochlea from the next is called the interscalar septum.(4)
Fig. 3
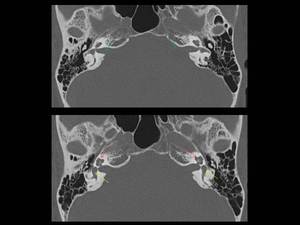
Fig. 4: Axial CT image showing normal anatomy of internal auditory canal (green arrows), cochlea (red arrows) and vestibule (yellow arrows)

Fig. 5: Coronal reconstruction CT image showing normal anatomy of cochlea (red arrows), semicircular canal (yellow arrows) and vestibule (green arrows)
Membranous Labyrinth
The interconnecting spaces actually within the membranous labyrinth constitute the endolymphatic cavity.
The membranous labyrinth consists of the cochlear duct,
the vestibular sense organs,
the endolymphatic duct and sac,
the round window membrane,
and the vascular system.
Cochlear Duct
The cochlear duct is a spiral tube lying within the cochlea and attached to its outer wall.
The cochlear duct is a blind pouch; it cleaves the perilymphatic space within the bony labyrinth,
dividing it into two portions,
the scala vestibule and the scala tympani.
The cochlear duct is triangular,
its roof being formed by Reisner’s membrane,
its outer wall by the endosteum lining the bony canal,
and its floor by the basilar membrane and the outer part of the osseous spiral lamina.
It contains the organ of Corti,
which is the site of placement of the supporting and sensory (hair) cells that mediate hearing.
Endolymphatic Duct and Sac
The endolymphatic duct begins within the vestibule as a dilated portion,
the endolymphatic sinus.
It arises at the confluence of the utricular and saccular ducts.
As it leaves the vestibule,
it narrows into an isthmus and passes into the vestibular aqueduct,
located near the crus common.
As the aqueduct turns caudally to approach the dural opening of the vestibular aqueduct,
the membranous duct (within the bony aqueduct) widens again into the flat endolymphatic sac.
The intraosseous part of the sac fills most of the vestibular aqueduct.
The remainder of the sac protrudes from the inferior aperture of the aqueduct and lies between the periosteum of the petrous bone and the dura mater.
The sac is not one compartment but rather a complex system of connecting channels.
(4)
IMAGING ANATOMY OF VESTIBULOCOCHLEAR NERVE:
Vestibulocochlear nerve carries special afferent fibers for hearing (the cochlear component) and balance (the vestibular component).
It enters the lateral surface of the brainstem,
between the pons and medulla,
after exiting the temporal bone through the internal acoustic meatus and crossing the posterior cranial fossa.
Inside the temporal bone,
at the distal end of internal acoustic meatus,
the vestibulocochlear nerve divides to form,
· Cochlear nerve
· Vestibular nerve
The vestibular nerve enlarges to form the vestibular ganglion,
before dividing into superior and inferior parts,
which distribute to the three semicircular ducts and utricle and saccule.
The cochlear nerve enters the base of the cochlea and passes upwards through modiolus,
the ganglion cells of the cochlear nerve are in the spiral ganglion at the base of the lamina of modiolus as it winds around the modiolus.
Branches of the cochlear nerve pass through the lamina of modiolus to innervate the receptors in the spiral ganglion.
Fig. 6

Fig. 6: Axial 3D FIESTA showing normal cochlear and vestibular nerve (white arrows) on both sides, vestibule (yellow arrow) and lateral semicircular canal (LSCC) (red arrow)
References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012
Fig. 7
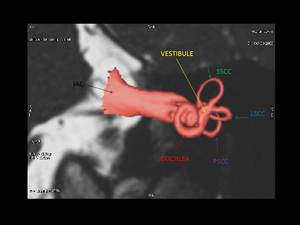
Fig. 7: Axial 3D reconstruction image showing internal auditory canal (black arrow), cochlea (red arrow), vestibule (yellow arrow), superior semicircular canal (SSCC, green arrow), lateral semicircular canal (LSCC, blue arrow), posterior semicircular canal (PSCC, purple arrow)
References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012
Fig. 8
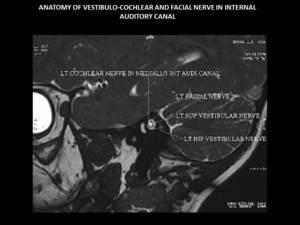
Fig. 8: Left oblique para-sagittal (3D FIESTA sequence) view showing vestibulo-cochlear and facial nerve in internal auditory canal.
References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012
HRCT AND MRI APPEARANCE OF COCHLEAR PATHOLOGIES
Jackler et al.,
1987 (3) classified congenital bony cochlear malformations as Michel deformity,
cochlear aplasia,
common cavity,
cochlear hypoplasia,
and incomplete partition (IP; Mondini dysplasia).
Sennaroglu & Saatci et al.,
2002 (5) proposed a new classification system that divided incomplete partition (IP) into subcategories: IP type I (cystic cochlear malformation) and IP type II (classic Mondini dysplasia).
Phelps used the term pseudo-Mondini for a dysplastic cochlea with a dilated basal turn,
and confined the originally described Mondini dysplasia to a normal basal cochlear turn and deficient inter scalar septum for the distal 1 ½ turns.
Moreover,
he emphasized that if the basal turn is intact,
some hearing will remain,
and there will be no risk of a major fistula (6).
Relative incidence of cochlear malformations:
|
Malformation
|
Incidence (%) |
|
Incomplete partition (Mondini's dysplasia)
|
55 |
|
Common cavity
|
26 |
|
Cochlear hypoplasia
|
15 |
|
Cochlear aplasia
|
3 |
|
Complete labyrinthine aplasia (Michel's aplasia)
|
1 |
Malformation of the inner ears may be associated with normal hearing.
This is especially in the case for semi-circular canal (SCC) anomalies.
Vestibular symptoms,
which occasionally are severe,
are present in approximately 20% of patients.
A wide variety of morphologic patterns of inner ear malformation has been observed radiographically and may involve the cochlea,
SCCs,
or vestibular aqueduct (VA).
Other anomalies cannot be explained by a premature arrest in development alone and appear to arise from an aberrant embryologic process.
An example of this type of anomaly is a cochlea of normal length but abnormal size or coiling geometry.
In humans,
the inner ear is of adult size at birth and shows strikingly little variation in size among individual patients.
Between the fourth and fifth weeks of development,
the spheric otocyst develops three buds that ultimately form the cochlea,
SCCs,
and VA.
An inner ear malformation may be limited to one of these anlages,
may involve a combination of two,
or may even affect all three.
Co-existence of deformities involving the cochlea,
SCCs,
and VA has several possible explanations: (1) the anomaly is genetically predetermined; (2) an insult to the embryo occurred before the fifth week; or (3) each of the buds was susceptible to some teratogenic influence at a later stage of development.
A majority of inner ear malformations are bilateral and symmetrical.
In cases in which radiographs detect an anomaly on only one side,
the opposite “normal” inner ear has a hearing loss in approximately 50% of cases.
MALFORMATION OF INNER EAR:
MICHEL APLASIA:
Also known as complete labyrinthine aplasia is a rare congenital inner ear abnormality,
accounting for approximately 1% of cochlear bony malformations.
This condition is defined as complete absence of inner ear structures and is caused by developmental arrest of otic placode early during the third week of gestational age.
Fig. 9
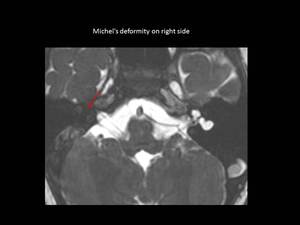
Fig. 9: Axial 3D FIESTA showing Michel’s deformity on right side (red arrow) in the form of complete absence of inner ear structures.
References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012
COCHLEAR APLASIA:
Failure of cochlea development late in the third week of gestation results in this condition.
COMMON CAVITY:
In common cavity malformation,
developmental arrest occurs at the fourth week of gestation and is defined as a single cavity that represents the undifferentiated cochlea and vestibule.
Fig. 10
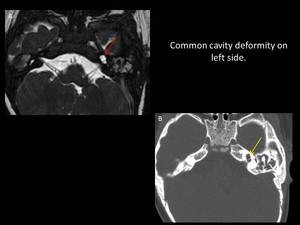
Fig. 10: Image A: Axial 3D FIESTA showing common cavity deformity on left side (red arrow), Image B: Axial CT of the same patient showing common cavity deformity (yellow arrow) on left side.
References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad, 2012
INCOMPLETE PARTITION I:
Incomplete partition I is also known as cystic cochlea vestibular malformation,
where the cochlea has no bony modiolus,
resulting in an empty cystic cochlea This is accompanied by a dilated cystic vestibule with developmental arrest at the fifth week of gestation (9).
INCOMPLETE PARTITION II:
In this group,
the cochlea consists of 1 ½ turns; the apical and middle cochlea turns are undifferentiated and form a cystic apex .
The vestibule is normal while the vestibular aqueduct is always enlarged.
Developmental arrest occurs at the seventh week of gestation.
Fig. 11
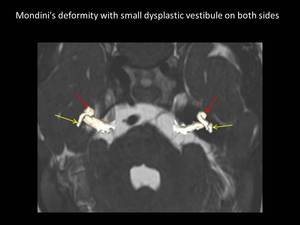
Fig. 11: Axial 3D FIESTA with superimposed reconstructed 3D image showing Mondini’s deformity (red arrows) and small dysplastic vestibule (yellow arrows) on both sides.
References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012
LABYRINTHITIS OSSIFICANS:
Labyrinthitis ossificans represents pathologic ossification of the membranous labyrinth as a response to an insult to the inner ear.
It occurs as the result of a healing reaction,
and generally occurs secondary to an inflammatory process such as infection (post meningitis),
trauma or any other tumorous processes.
This condition leads to a sensorineural hearing loss,
and may prevent or complicate cochlear implantation.
(10,11)
Fig. 12 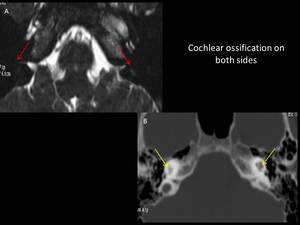
Fig. 12: Image A:Axial 3D FIESTA showing loss of normal fluid filled spaces of membranous labyrinth on both sides (red arrows), Image B:Axial CT scan of same patient showing ossification of cochlea and vestibule on both sides (yellow arrows)
References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012
ANOMALIES OF THE EIGHTH NERVE:
Hypoplasia and aplasia of the eighth nerve are often,
but not inevitably,
associated with congenital narrowness or even absence of the IAC.
Similarly,
although eighth nerve maldevelopment frequently accompanies malformation of the inner ear,
the presence of a normal cochlea and semicircular canals does not guarantee normal development of the audiovestibular nerve.
High-resolution,
thin-section MRI with T2-weighted sequences currently is the best means of assessing the fine anatomy of the eighth nerve in the IAC.
The internal auditory canal frequently is normal.
Fig. 13
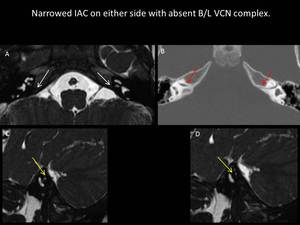
Fig. 13: Image A: Axial 3D FIESTA showing absent vestibulo-cochlear nerve (VCN) on both sides (white arrows), Image B: Axial CT scan showing narrowed internal auditory canal (IAC) on both sides (red arrows), Image C and D: Right and left oblique parasagittal (3D FIESTA) views showing absent VCN (yellow arrows)
References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012
SEMICIRCULAR CANAL ABNORMALITIES:
The most commonly recognised semicircular canal abnormality is a short lateral semicircular canal being confluent with the vestibule.
Ears with malformations limited to the vestibular system often have normal or near-normal hearing.
When the cochlea also is abnormal,
sensory hearing levels tend to be impaired,
to a variable degree.
The SCC dysplasia appears to have an association with conductive hearing loss,
presumably because of inner ear micromechanical factors rather than stapes fixation (12).
The LSCC malformation is associated with SNHL and conductive hearing loss (CHL) varied from mild to profound but did not correlate with the severity of LSCC malformation.
Fig. 14
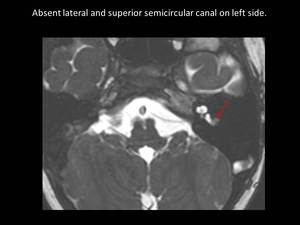
Fig. 14: Axial 3D FIESTA showing absent lateral semicircular canal (SCC) and superior SCC on left side (red arrow)
References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012
ENLARGED VESTIBULAR AQUEDUCT (VA):
Enlargement of the VA is the most common radiographically detectable malformation of the inner ear (3,5).
Enlargement of the VA is diagnosed when its diameter exceeds 2 mm,
although enlarged VAs may exceed 6 mm in width.
In many cases,
VA enlargement accompanies malformation of the cochlea or SCC.
It also may be the sole radiographically detectable abnormality of the inner ear in a child with hearing loss.
This condition is commonly referred to as the large VA syndrome.
The advent of high-resolution CT in the axial plane has made assessment of the VA much easier.
Normally the vestibular aqueduct is not seen or is appreciated as only a lucent line.
The vestibular aqueduct was considered enlarged if the external pore was greater than 2 mm.
Fig. 15
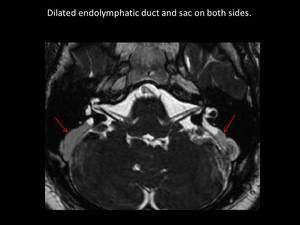
Fig. 15: Axial 3D FIESTA showing dilated endolymphatic duct and sac on both sides (red arrows)
References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012
INTERNAL AUDITORY MEATUS:
It can be narrow or wide.
A congenitally large canal may be an incidental finding in healthy individuals When a large internal auditory canal (IAC) (larger than 10 mm in diameter) accompanies a malformation of the inner ear,
it does not,
as an independent variable,
correlate with the level of hearing.
Primary importance of detecting enlargement of the IAC is its association with spontaneous CSF leak and the occurrence of gusher during stapes surgery.
 A narrow IAC may indicate a failure of eighth cranial nerve development.
When a patient has normal facial function and an IAC less than 3 mm in diameter,
it is likely that the bony canal transmits only the facial nerve .
A narrow IAC may accompany inner ear malformations or may be the sole radiographically detectable anomaly in a deaf child.
A narrow IAC was considered a relative contraindication to cochlear implantation,
because it suggests that the eighth nerve may be insufficiently developed to conduct an auditory signal,
but now with the help of MRI the cochlear nerve can be studied carefully before planning for surgery.
A narrow IAC may indicate a failure of eighth cranial nerve development.
When a patient has normal facial function and an IAC less than 3 mm in diameter,
it is likely that the bony canal transmits only the facial nerve .
A narrow IAC may accompany inner ear malformations or may be the sole radiographically detectable anomaly in a deaf child.
A narrow IAC was considered a relative contraindication to cochlear implantation,
because it suggests that the eighth nerve may be insufficiently developed to conduct an auditory signal,
but now with the help of MRI the cochlear nerve can be studied carefully before planning for surgery.
Fig. 16
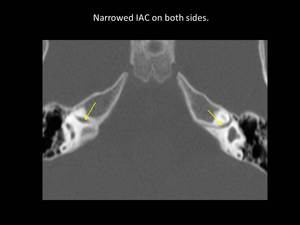
Fig. 16: Axial CT scan showing narrowed internal auditory canal (IAC) on both sides (yellow arrows)
References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012
HRCT depicts the minute details of dysplastic or ossified cochlea,
enlarged vestibular aqueduct,
high-riding jugular bulb,
aberrant facial nerve course and abnormal bony structures.
However absence of vestibule-cochlear nerve (VCN) cannot be detected accurately on HRCT.
MRI allows visualization of fluid-filled spaces of the inner ear,
early stages of fibrosis,
VCN,
and brain. However,
complete ossification of cochlea and labyrinth cannot be detected well on MRI.
Following are the list of imaging findings what the cochlear implant surgeon wants to know from the reporting radiologist.
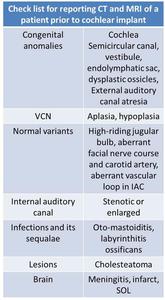
Table 1: Check list for reporting CT and MRI of a patient prior to cochlear implant

 Congenital malformations of the inner ear: a classification based on organogenesis. Laryngoscope 97:2–14.")
 Anatomy and physiology- the unity of form and function. 3rd ed. New York: McGraw-Hill;")
 eDoctorOnline.com")
, cochlea (red arrows) and vestibule (yellow arrows)")
, semicircular canal (yellow arrows) and vestibule (green arrows)")
 on both sides, vestibule (yellow arrow) and lateral semicircular canal (LSCC) (red arrow) References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012")
, cochlea (red arrow), vestibule (yellow arrow), superior semicircular canal (SSCC, green arrow), lateral semicircular canal (LSCC, blue arrow), posterior semicircular canal (PSCC, purple arrow) References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012")
 view showing vestibulo-cochlear and facial nerve in internal auditory canal. References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012")
 in the form of complete absence of inner ear structures. References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012")
, Image B: Axial CT of the same patient showing common cavity deformity (yellow arrow) on left side.
References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad, 2012")
 and small dysplastic vestibule (yellow arrows) on both sides.
References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012")
, Image B:Axial CT scan of same patient showing ossification of cochlea and vestibule on both sides (yellow arrows)
References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012")
 on both sides (white arrows), Image B: Axial CT scan showing narrowed internal auditory canal (IAC) on both sides (red arrows), Image C and D: Right and left oblique parasagittal (3D FIESTA) views showing absent VCN (yellow arrows) References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012")
 and superior SCC on left side (red arrow)
References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012")

References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012")
 on both sides (yellow arrows)
References: Department of Radiology, B J Medical College and Civil Hospital/Gujarat University, Ahmedabad 2012")
