| A.- FINDINGS IN DIFFERENT LESIONS.
RADIO-PATHOLOGIC CORRELATION. |
Mucinous breast carcinoma accounts for 1-6% of primary breast carcinomas,
with higher prevalence in older women,
usually older than 55-60 years at diagnosis,
and better prognosis than usual breast carcinoma.
The hystopathologic definition is a tumor with a mucinous component of 50% or more. According to World Health Organization (WHO) two subtypes may be found: pure and mixed mucinous breast carcinoma.
The mixed type contains 50-90% of mucinous component and the pure type more than 90%.
Mucinous breast carcinoma commonly appears on mammograms as well-circumscribed,
round,
or lobular masses,
although sometimes focal asymmetry may appear.
A high-density mass is the most frequent feature,
either circumscribed or with irregular or indistinct margins.
On US they are usually solid masses,
predominantly hypoechoic with lobulated margins and heterogeous internal echotexture.
The presence of posterior acoustic enhancement beneath a solid hypoechoic breast lesion should raise suspicion of mucinous carcinoma.
The MR features of pure mucinous breast carcinoma,
may also resemble benign lesions with homogenous high-signal intensity on T2-weighted imaging due to mucinous component,
and T1 signal intensity varies from low to high depending on protein percentage.
Enhancement patterns are usually type I curves (gradual enhancement) or type II (plateau-type),
or may be those of a malignant lesion with rim or heterogeneous enhancement.
The ADC values of pure mucinous tend to be greater than those of benign lesions and other malignant tumors.
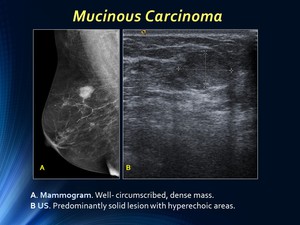
Fig. 1: Case 1: Mammogram and US: Mucinous Carcinoma
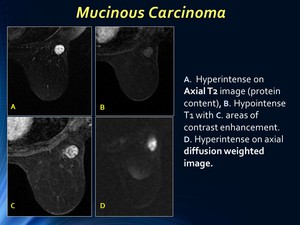
Fig. 2: Case 1: MR: Mucinous Carcinoma

Fig. 3: Case 2: Mucinous Carcinoma
Medullary carcinoma of the breast accounts for less than 5% of invasive breast cancer. It presents in younger women and has a favorable prognosis.
The WHO definition consists of “a well-circumscribed carcinoma with poorly differentiated cells,
scant stroma and prominent lymphoid infiltration”.
Histopathologic diagnostic criteria include: lymphoplasmacytic infiltration,
noninvasive microscopic circumscription,
syncytial growth pattern >75%,and grade 2 or 3 nuclei.
It may be a subtype of basal breast cancers.
Immunohistochemical features are variable,
usually negative estrogen,
progesterone,
and HER2 receptors,
but positive estrogen and progesterone receptors have been reported.
On mammograms round or oval masses with well-circumscribed margins,
and no calcifications are usually depicted.
On US well-circumscribed hypoechoic nodules appear,
sometimes with cystis areas.
On MR an oval or lobular mass with circumscribed margins and usually homogeneous due to high cellularity cause by lymphoplasmacytic infiltrates.
After intravenous gadolinium rim enhancement with or without enhancing internal septations is usually found.
Contrast enhancement shows a rapid initial increase and a washout or plateau pattern on delayed phase.
A hypointense rim on T2-weighted images may be found in certain cases.

Fig. 4: Medullary Carcinoma: Mammogram and US. Case 1

Fig. 5: Medullary Carcinoma: MR, gross specimen and H-E stain. Case 1
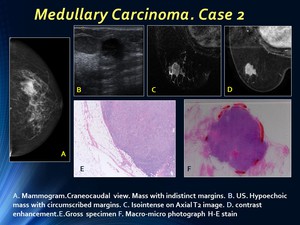
Fig. 6: Medullary carcinoma. case 2
Papillary carcinoma of the breast accounts for 1-2% of breast carcinomas and appears in older women,
about 50-60 years old at diagnosis.
The prognosis tends to be good as it is most frequently intraductal carcinoma,
bit infiltrating carcinoma may appear.
Two different types may be found: papillary carcinoma in situ,
which is the most frequent type and may be intraductal or intracystic,
and infiltrating papillary carcinoma,
a rare condition.
At histopathology this tumor is characterized by round,
well-defined nodules with exclusively or predominantly papillary configuration.
They are composed of low-grade ductal cells separated by fibrovascular cores or vascular channels,
which appear within the septa in intracystic lesions.
Hemorrhage is frequently present.
Imaging findings of intracystic papillary carcinoma are those of a cystic lesion with solid area which most frequently appears in the retroareolar area.
On mammograms well-circumscribed nodules,
sometimes with satellite lesions are found.
On US a complex mass with different components is depicted,
usually with cystic area and posterior acoustic enhancement.
MR depicts multicystic nodules,
with hyperintense areas on T1 weighted images due to hemorrhage and gadolinium enhancement of walls and septa,
typically with washout pattern (type III curves).
Invasive papillary carcinoma features are similar,
on mammograms and US a mass with smooth margins,
but which sometimes may be ill-defined,
and most frequently complex but sometimes solid.
On MR margins are usually circumscribed or sometimes ill-defined and internal enhancement tends to be homogeneous sometimes with hypointense central area.
A washout pattern (type III curve) is usually found.
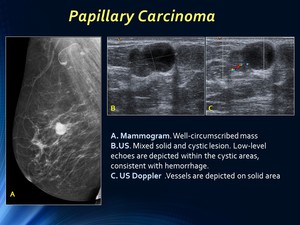
Fig. 7: Papillary Carcinoma: mammogram and US
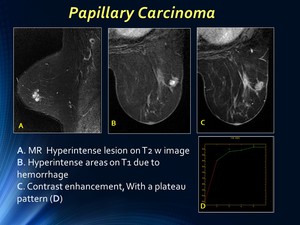
Fig. 8: Papillary Carcinoma: MR
| 4.
MALIGNANT PHYLLODES TUMOR.
Fig. 9 |
Malignant phyllodes tumor accounts for 1% of malignant breast tumors.
It appears in medium age women (35-55 years).
Its definition is a fibroepithelial neoplasm,
with epithelial component and a connective stroma,
in which stroma is the neoplastic component determining agressivity.
There are three different subtypes of phyllodes tumors: benign,
borderline and malignant.
The histopathological features of malignant phyllodes tumors include hypercellular stromal overgrowth ,
stromal cellular pleomorphism and a number of mitosis greater than five per 10 high-power fields.
Presenting lesion at mammography is usually a high-density mass with smooth margins without microcalcifications.
Malignant Phyllodes tumors tend to grow rapidly and size tends to be bigger at presentation than benign ones.
On US a well-circumscribed,
lobulated mass,
predominanty hypoechoic heterogeneous with frequent cystic areas and sometimes thick septa.
Cystic areas are more frequent in malignant phyllodes tumors than in benign phyllodes tumors and fibroadenomas.
MR imaging findings include large masses with smooth margins,
cystic areas hyperintense on T2-weighted images and irregular walls.
Areas of high T1 signal may appear due to hemorrhage.
Contrast enhancement is depicted on solid components,
walls and septa,
usually with a washout pattern (type III curve).
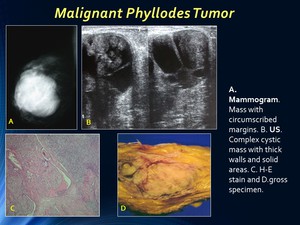
Fig. 9: Malignant Phyllodes Tumor
| 5.
LOW GRADE INFILTRATING CARCINOMA,
IN SITU DUCTAL CARCINOMA.
Fig. 10 |
Any ductal carcinoma may appear as circumscribed on mammogram.
Circumscribed carcinoma is less frequently seen than typical spiculated carcinoma but this benign appearance may be caused by invasive ductal carcinoma and some in situ ductal carcinoma.
Circumscribed lesions on mammograms and on US very hypoechoic lesions sometimes mimicking a cyst.
Parameter settings are important in order to distinguish a solid lesion.
MR usually helps by showing lesions with contrast enhancement and type III washout curves.
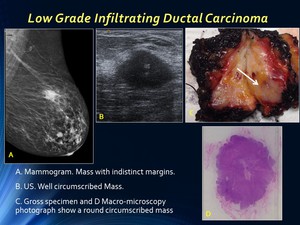
Fig. 10: Low Grade Infiltrating Ductal Carcinoma
B.- FINDINGS IN DIFFERENT IMAGING METHODS.
DIFFERENTIAL DIAGNOSIS
|
Breast malignancies may present with non-agressive features.
All breast masses should be carefully assessed,
as they may be tricky and be malignant in spite of a benign-looking appearance.
Aditional clinical details should be always considered.
Gradually progressive swelling,
usually rapidly is the most frequent presenting symptom of malignant agressive tumors.
Looking for subtle findings on mammograms and comparing with previous studies are important clues,
a new lump or a mass on mammograms,
in spite of its innocent appearance may hide a malignancy.
Medullary,
mucinous and papillary carcinoma and malignant phyllodes tumors usually present with large cystic areas due to necrosis or colloid content.
On US they are complex masses mixed solid and cystic masses or cysts with nodular appearing solid area.
Cystic masses with more than 50% solid area are suspicious,
but even smaller solid areas may be malignant.
The solid area should be biopsied,
the cystic area may be necrosis.
US-guided techniques should reach the solid area,
and sometimes emptying cystic area with fine needle aspiration biopsy (FNAB) prior to biopsy may be helpful.
Very hypoechoic masses may also be tricky by resembling a cyst on US.
Careful adjusting US settings is mandatory in order to avoid false diagnosis.

Fig. 11: US Tips, tricks and Keys
MR helps in the evaluation of breast masses,
specially useful in difficult cases.
Analysis of the lesion signal intensity on T2-weighted MR images,
assessment of the enhancement pattern,
and kinetic curve help in differential diagnosis between malignant and benign well-circumscribed breast lesions.
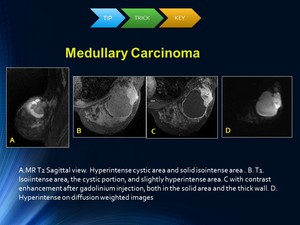
Fig. 12: MR Tips, tricks and keys












