ECR 2015 / C-1066
Cholecystitis - pearls and pitfalls on ultrasound
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2015
Poster Number:
C-1066
Type:
Educational Exhibit
Keywords:
Gastrointestinal tract, Abdomen, Ultrasound, Ultrasound-Colour Doppler, Diagnostic procedure, Education, Acute, Artifacts, Calcifications / Calculi
Authors:
J. C. Ruivo Rodrigues, B. Rodrigues, C. F. R. C. Ribeiro, H. Nunes Correia, A. Figueiredo, N. M. P. Ribeiro; Viseu/PT
DOI:
10.1594/ecr2015/C-1066
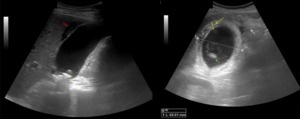
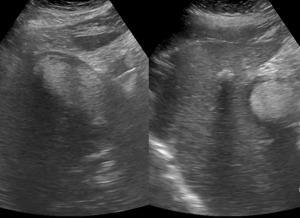
, wall thickening (yellow arrow), gallstone (green arrow), echogenic inflamed fat (white arrow) and pocket of oedema fluid (red arrow).")
Fig. 1:
Ultrasound images showing acute calculous cholecystitis with pericholecystic...
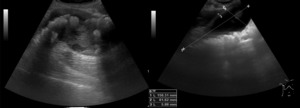
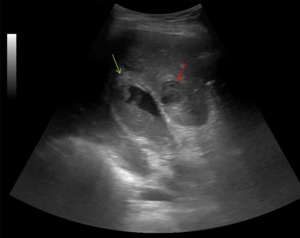
 and diffuse mural thickening wall (5.88 mm), in gallbladder cancer.")
Fig. 3:
Ultrasound images showing intraluminal echogenic mass lesion, gallbladder...

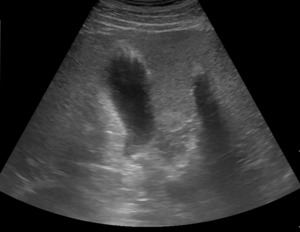
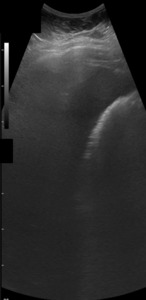
Fig. 2:
Ultrasound image showing fundal mural thickening of the gallbladder and...

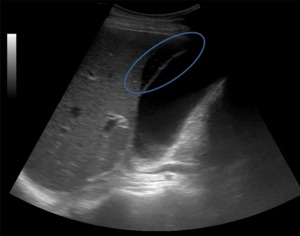
Fig. 4:
Ultrasound image showing pericholecystic fluid collection with a thin anechoic...

Fig. 5:
Ultrasound image showing pericholecystic fluid collection with irregularly...

Fig. 6:
Ultrasound image showing acute acalculous cholecystitis with pericholecystic...
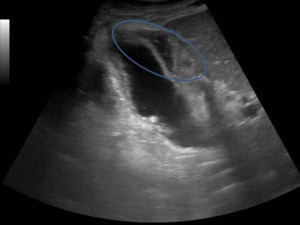
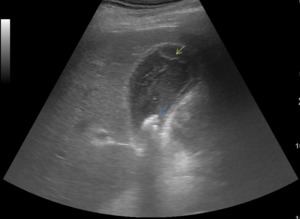
 appearing as a linear intraluminal echo, echogenic material within the lumen and gallstones (blue arrow).")
Fig. 7:
Gangrenous cholecystitis: sloughed membrane (green arrow) appearing as a linear...
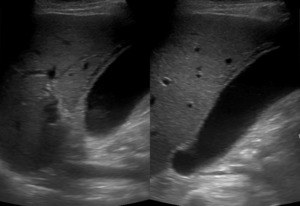
 – Ultrasound image showing presence of a distended gallbladder, with diffuse wall thickening and filled with echogenic material with a higher echogenicity than sludge representing hemorrhage.")
Fig. 8:
Hemorrhagic Cholecystitis (HC) – Ultrasound image showing presence of a...
, with a pericholecystic abscess (red arrow).")
Fig. 9:
Ultrasound image showing subacute perforation in the fundus (green arrow), with...
.")
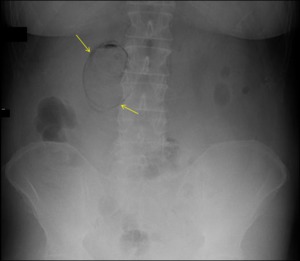
Fig. 10:
Abdominal radiogram showing dilatated bowel loops, in relation with intestinal...
.")
Fig. 11:
Ultrasound image showing abscess in the gallbladder fossa (red wheel).
.")
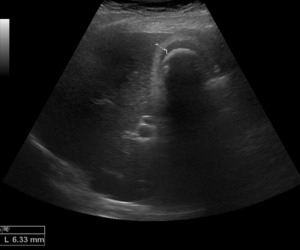
Fig. 12:
Abdominal radiogram showing a radiolucency bordering the bile fossa and inside...
.")
Fig. 13:
Ultrasound image showing absence of a normal gallbladder with highly echogenic...
, due to fibrosis, presence of gallstone, which produce a posterior acoustic shadowing with fibrosis of the wall (WES complex).")
Fig. 14:
Ultrasound image showing chronic inflammation of the gallbladder wall (6,33...
) partial layer of mineralisation outlining the gallbladder wall. Ultrasound image showing (b)) an hyperechoic semilunar structure with complete posterior acoustic shadowing.")
Fig. 15:
Abdominal radiogram showing (a)) partial layer of mineralisation outlining the...

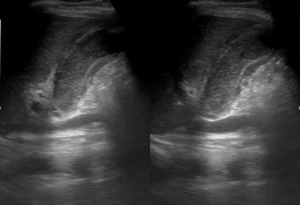
Fig. 16:
Ultrasound images showing diffuse gallbladder wall thickening, with intramural...
.")
Table 1:
Correlation between sonographic characteristics and pathophysiology of...
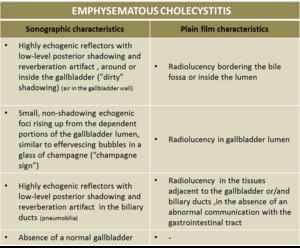
 and plain film (4) characteristics of the emphysematous cholecystitis.")
Table 2:
Correlation between sonographic (1) and plain film (4) characteristics of the...
.")
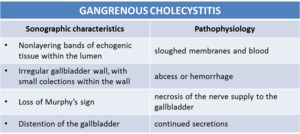
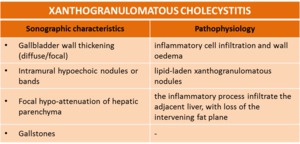
Table 3:
Correlation between sonographic characteristics and pathophysiology of the...