Generalities and procedure details
Muscle strains ususally occur (92%) among 4 main groups of lower limb muscles in football players (37% hamstrings,
23% adductors,
19% quadriceps,
13% calf) (1).
Every muscle has peculiar anatomy and conjunctive structure,
which causes a unique lesional spectrum.
Knowledge can lead to better identification of these lesions.
Ultrasound examination must be performed first between the 2nd and the 7th day to avoid underestimating a "fresh" isoechoic lesion.
MRI can be added in case of clinico-ultrasound conflict,
suspicion of complete muscular rupture or tendinous avulsion.
Standard protocol should include T1-weighted imaging in one section (usually axial) and STIR or T2 whith fat saturation (FS) weighted in at least two sections.
Some authors (5)(6)(7)(8) consider ultrasound superior to MRI while others (9)(10) agree on similar performance.
The main benefit of ultrasound is to study muscular contractility and allow imaging guided treatments (hematoma drainage) at the same time.
Ultrasonography also allows in most cases to differentiate blurred hyperemic recent injuries (Doppler is classically positive from the 3rd day) from well-defined older injuries.
The main asset of MRI is its excellent sensibility,
its less operator dependability and its better deep muscles exploration.
Hamstrings
Anatomy
There are two proximal tendons inserted on ischium:
- Conjoint tendon,
posteromedial then lateral,
which extends in a sagittal aponeurotic septum between long head of biceps femoris and semitendinosus,
- Semimembranosus tendon,
anterolatéral then medial which expends into an aponeurosis,
from which start muscular fibers.
Each hamstring has an intramuscular conjunctive wall:
- Long head of the biceps femoris: a frontal wall,
- Semitendinosus: a sagittal sigmoid septum,
very usefull as ultrasound reference point,
- Semimembranosus: frontal wall.
The long head of the biceps femoris terminates on the short head of the biceps femoris aponeurosis and on the distal tendon.
The semitendinosus and the semimembranosus each have a distal tendon.
Ususal lesions
In footballers,
83% of muscle strains concern biceps femoris,
12% semimembranosus and 5% semitendinosus (11).
In the superior third of the thigh:
- Lesions of tendon conjoint or semimembranosus
In the middle third of the thigh:
- Lesions of frontal septum of biceps femoris or semimembranosus
In the inferior third of the thigh:
- Lesions of biceps femoris are often peripheral along the aponeurotic septum between the long and the short head.
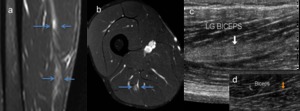
Fig. 4: Central myofascial lesion (« 2m ») of the long biceps femoris. (a-b): Hypersignal (arrows) on sagittal and axial STIR weighted MRI. (c) Hyperechoic area on sagittal US only on one side of the intramuscular frontal conjunctive wall (arrow). (d) Normal aspect of the conjunctive wall on the other side (arrow).
References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014

Fig. 5: Lesion focused on the distal part of the frontal conjunctive wall of the long biceps femoris (“2c”). (a-b): Hypersignal (arrows) on sagittal and axial STIR weighted MRI. (c) US (sagittal view) hyperechoic area on both sides of the same conjunctive wall, which appears, blurred.
References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014

Fig. 6: Rupture with hematoma of the peripheral myofascial junction of the long head of the biceps femoris (on the short head of the biceps femoralis) (“3c”). (a-b). Axial and sagittal STIR weighted MRI: Hypersignal and rupture of perimuscular conjunctive wall (c). US correlation with collected hematoma and positive power-Doppler.
References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014
Adductors
Anatomy
There are five adductors to posterior:
- Adductor longus arises from a tendon inserted on the inferior surface of the pubis which extends in a frontal intramuscular septum
- Gracilis has myoperiosteous insertion just behind
- Pectineus extends under the femoral vessels
- Adductor brevis and adductor magnus arise from a myoperiosteous insertion on the iliopubic line
Usual lesions
- Central lesion of adductor longus along the frontal conjunctive wall
- On the sagittal conjunctive septum
- On the peripheral myofascial junction

Fig. 7: Lesion focused on the frontal conjunctive wall of the adductor longus (“2c”). Sagittal view US: (a) Hyperechogenicity on the both side of the frontal conjunctive wall of the right adductor longus (arrow) compared with healthy side (thin conjunctive wall) (b).
References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014

Fig. 8: Peripheral myofascial lesion (« 2m ») of left adductor longus. (a-b) Coronal and axial STIR weighted MRI: Hypersignal of muscle fibers on one side of epimysium of the adductor longus. (c) Ultrasound correlation.
References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014
Rectus femoris
Anatomy
It is a bipenned muscle from two proximal tendons:
- Direct tendon inserts on the anterior inferior iliac spine spine
- Reflected tendon inserts above the acetabulum
This muscle has a sagittal intramuscular septum extended on two thirds of the muscle
Usual lesions
- Anterior inferior iliac spine avulsion,
usually occurs in the teenage years and what is frequently observed is a cicatrization in the form of a hypertrophic ossification whitout functional impact
- On the sagittal conjunctive septum
- On the peripheral myofascial junction

Fig. 9: Lesion focused on the sagittal conjunctive wall of the rectus femoris (“2c”). (a-b) Ultrasound: Hyperechogenicity in muscle fibers on the both sides of the sagittal conjunctive wall (double arrows) compared with healthy side. (c-d) Axial and coronal STIR weighted MRI: hypersignal in muscle fibers (low ked focused disorganization) on the both sides of the sagittal conjunctive wall (simple arrows)
References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014

Fig. 10: Peripheral myofascial lesion « 3m » of right rectus femoris
(a-b). Axial and coronal MRI STIR weighted: desinsertion of muscle fibers (arrows). (c) US correlation where hematoma is well-seen (arrow).
References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014
"Tennis leg"
Anatomy
Triceps surae muscle is composed of:
- Medial and lateral gastrocnemii which arise from femoral condyles and progress superficially up to their distal and deep aponeurosis
- Soleus,
which arises from fibrous arch between tibia and fibula,
progress deep to gastrocnemii and attaches on a superficial aponeurosis.
It has one main proximal sagittal conjunctive wall and two distal frontal conjunctive walls.
- Plantaris arises from lateral supracondylar area with an oblique course,
low and medial.
Calcaneus tendon is made of the union of distal aponeurosis of gastrocnemii and soleus.
Plantaris inserts medially relatively to it.
Usual lesions
"Tennis leg" is a polymorphic traumatic lesion of the calf:
- Distal myoaponeurotic desinsertion of medial gastrocnemius: most common,
represent 67% of "tennis leg" (12); a hematoma can be seen between distal aponeurosis of medial gastrocnemius and soleus (needing US-guided evacuation).
- Aponeurotic detachment between gastrocnemius and soleus without collected hematoma,
muscular abnormalities or conjunctive rupture (grade 2c).
- Myoconjunctive or only conjunctive soleus desinsertion: conjunctive structures of soleus are complex,
defining a polymorphic lesional spectrum.

Fig. 11: Ultrasound imaging of the calf: (a) Distal myofascial desinsertion of medial gastrocnemius (3m); (b) healthy side for comparison
References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014

Fig. 12: Aponeurotic detachment between medial gastrocnemius and soleus (“2c”). (a-b) Thickening of the conjunctive wall without muscular abnormalities compared with healthy side. (c-d) Axial and sagittal T2- FS weighted MRI: Thickening and hypersignal of the conjunctive wall without muscular abnormalities
References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014

Fig. 13: US (sagittal view): Hematoma between distal aponeurosis and muscle fibers of medial gastrocnemius (“3m”)
References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014

 of the long biceps femoris. (a-b): Hypersignal (arrows) on sagittal and axial STIR weighted MRI. (c) Hyperechoic area on sagittal US only on one side of the intramuscular frontal conjunctive wall (arrow). (d) Normal aspect of the conjunctive wall on the other side (arrow). References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014")
. (a-b): Hypersignal (arrows) on sagittal and axial STIR weighted MRI. (c) US (sagittal view) hyperechoic area on both sides of the same conjunctive wall, which appears, blurred. References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014")
 (“3c”). (a-b). Axial and sagittal STIR weighted MRI: Hypersignal and rupture of perimuscular conjunctive wall (c). US correlation with collected hematoma and positive power-Doppler. References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014")
. Sagittal view US: (a) Hyperechogenicity on the both side of the frontal conjunctive wall of the right adductor longus (arrow) compared with healthy side (thin conjunctive wall) (b). References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014")
 of left adductor longus. (a-b) Coronal and axial STIR weighted MRI: Hypersignal of muscle fibers on one side of epimysium of the adductor longus. (c) Ultrasound correlation. References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014")
. (a-b) Ultrasound: Hyperechogenicity in muscle fibers on the both sides of the sagittal conjunctive wall (double arrows) compared with healthy side. (c-d) Axial and coronal STIR weighted MRI: hypersignal in muscle fibers (low ked focused disorganization) on the both sides of the sagittal conjunctive wall (simple arrows) References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014")
. Axial and coronal MRI STIR weighted: desinsertion of muscle fibers (arrows). (c) US correlation where hematoma is well-seen (arrow). References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014")
 Distal myofascial desinsertion of medial gastrocnemius (3m); (b) healthy side for comparison References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014")
. (a-b) Thickening of the conjunctive wall without muscular abnormalities compared with healthy side. (c-d) Axial and sagittal T2- FS weighted MRI: Thickening and hypersignal of the conjunctive wall without muscular abnormalities References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014")
: Hematoma between distal aponeurosis and muscle fibers of medial gastrocnemius (“3m”) References: Department of Radiology, Pitié Salpetrière Hospital, Medical University of Paris/ France 2014")