Anatomy of the Thoracic Duct:
- Tubular structure extending from cisterna chyli at the the second lumbar vertebral body to the junction of the left subclavian and left interval jugular veins [1,2].
- Originates at the abdominal cisterna chyli,
extends along the posterior aspect of the aorta and right diaphragmatic crus,
and enters the thorax between the aorta and azygos vein.
- Courses through the posterior mediastinum deep to the esophagus and pericardium.
- Enters the superior mediastinum at the fifth thoracic vertebral body and extends posterior to the aortic arch and left subclavian artery.
- Crosses anterior to the subclavian and vertebral veins,
thyrocervical trunk,
and anterior scalene muscle in the neck.
- Drains into the junction of the left subclavian and left internal jugular veins.
- 2-5 mm in diameter [1].
- 38-45 cm in length [1].
- Carries 1-2 L of lymphatic fluid/day [1].
- 80% of lymphatic fluid is from intestinal and hepatic lymphatic ducts [1].
- See our exhibit entitled Illustration of Variable Thoracic Duct Anatomy for Thoracic Duct Embolization Pre-Procedure Planning for additional anatomic description.

Fig. 1: Schematic diagram demonstrating the normal course of the thoracic duct (solid green outline). Adapted from: Allaham AH, Estrera AL, Miller CC, Achouh P, Safi HJ. Chylothorax complicating repairs of the descending and thoracoabdominal aorta. Chest. 2006;130(4):1138-42.
Causes of Chylous Leaks and Indications for Thoracic Duct Embolization:
- Two mechanisms of chylous extravasation: (1) direct trauma to the lymphatic vessels and (2) occlusion of the thoracic duct with concurrent delicate collateral duct formation [3,4].
- Traumatic injury is the most common cause of chylous extravasation typically from thoracic,
cardiac,
or head and neck surgeries [5].
- 0.42% injury from general thoracic surgery [6].
- 3.9% injury from esophagectomy [7].
- Nontraumatic occlusion of the thoracic duct is less common,
but may arise from maligancies (lymphoma,
esophageal adenocarcinoma,
primary lung malignancies,
and mesothelioma),
systemic diseases and infections (sarcoidosis,
tuberculosis,
and Behcet's disease),
lymphatic vessel diseases (lymphangiomatosis and Gorham's disease),
congenital malformations,
and idiopathic cases [8].
- 42% nontraumatic obstruction from idiopathic causes [9].
- 27% nontraumatic obstruction from malignancies such as lymphoma [9].
- Low-output chylous leakage (<1000 mL/day) treated conservatively with diet [10].
- High-out chylous leakage (>1000 mL/day) treated with thoracic duct embolization or surgical ligation [11].
- Indications for thoracic duct embolization include: chylothorax,
chylopericardium,
and postoperative chylous wound leakage (less likely chylous ascites,
chyloptysis,
and chyluria).
Thoracic Duct Embolization Pre-Procedural Imaging:
- Magnetic resonance ductography including heavily T2-weighted axial and coronal images of the thoracoabdominal region.
-
Lymphangiography.
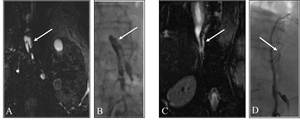
Fig. 2: Coronal T2-weighted magnetic resonance images (A and C) and corresponding lymphangiogram images (B and D) demonstrating dilated lymphatic channels in the retrocrural spaces and retroperitoneum (solid white arrows).
Thoracic Duct Intra-Procedural Techniques:
Cut-down,
Lymphatic Duct Isolation,
and Pedal Lymphangiography:
- Intravenous moderate procedural sedation is administered.
- Prophylactic administration of 1-2 g cefazolin is given for skin flora.
- 0.5-1 mL of methylene blue dye (American Regent,
Shirley,
New York) is injected intradermally into the first and second and third and forth web spaces of the toes to facilitate visualization of lymphatic vessels.
- Local anesthesia with 2% lidocaine is provided and a 2 cm incision is made along the dorsum of the foot.
- A lymphatic duct is identified,
tied with silk,
and cannulated with a 30-gauge lymphangiography needle (Cook,
Bloomington,
Indiana).
- Ethiodized oil (Ethiodol; Savage Laboratories,
Melville,
New York or Lipiodol UltraFluide,
Guerbet,
Roissy,
France) is infused at a rate of 8-10 mL/hour with a power injector into the lymphangiography needle.
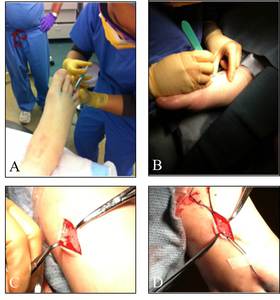
Fig. 3: Multiple images demonstrating the injection of methylene blue dye (A), creation of a longitudinal incision along the dorsum of the foot (B), and isolation of a lymphatic duct (C and D).
Lower Extremity Lymphangiography:
- Spot radiographs of the lower extremity are obtained every 15 minutes to monitor the progression of the ethiodized oil throughout the lower extremity.
- Evaluation is terminated when the ethiodized oil opacifies the cisterna chyli.
- Prophylactic administration of 500 mg levofloxacin is given for gastrointestinal flora.
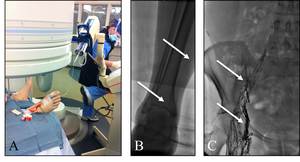
Fig. 4: Multiple images demonstrating the injection of ethiodized oil into the lymphatic system (A) and evaluation of its progression through the lower extremity (B) and pelvis (C) (solid white arrows).
Cisterna Chyli Access and Cannulization:
- Under fluoroscopic guidance,
the opacified cisterna chyli,
or prominent retroperitoneal duct,
is accessed using a 21-gauge 15 cm needle with an inner stylet using a right transabdominal approach.
- Access is confirmed by injection of 1 mL of iodinated contrast material.
- Once targeted,
the inner stylet is removed and an 0.018-inch guidewire (Boston Scientific,
Natick,
Massachusetts) is advanced through the thoracic duct and into the thorax.
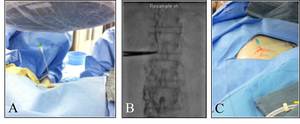
Fig. 5: Multiple images demonstrating the initial transabdominal access (A), continuous fluoroscopic monitoring to access the cisterna chyli (B), and guidewire placement into the thoracic duct (C).
Thoracic Duct Lymphangiography:
- A 3 F straight Slip-Cath microcatheter (Cook,
Bloomington,
Indiana) is advanced over the guidewire into the thoracic duct.
- The wire is removed and iodinated contrast is injected to evaluate the type of thoracic duct and the level and degree of contrast extravasation.
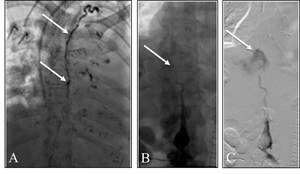
Fig. 6: Multiple lymphangiogram images demonstrating a normal appearing thoracic duct (A) (solid white arrows) and an abrupt cut off (B) with massive contrast extravasation (C) (solid white arrows) consistent with thoracic duct injury and leakage.
Thoracic Duct Embolization:
- Embolization coils are deployed proximally along the entire course of the thoracic duct.
- A 2:1 ethiodized oil and N-butyl cyanoacrylate glue (Codman and Shurtleff, Raynham,
Massachusetts) mixture with tantalum powder is used to complete the embolization of the distal thoracic duct and cisterna chyli.
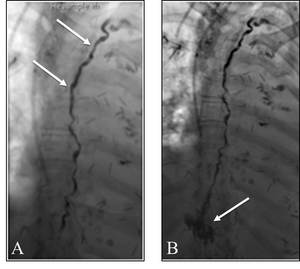
Fig. 7: Multiple images demonstrating the placement of embolization coils proximally (A) (solid white arrows) and N-butyl cyanoacrylate glue distally (B) (solid white arrows).
Thoracic Duct Embolization Success Rates:
- Overall technical success rate of 79% [12].
- Overall clinical success rate of 55-73.8% [13,14].
- Traumatic chylous leakage clinical success rate: 62% [12].
- Nontraumatic chylous leakage clinical success rate: 13% [12].
- Complication rates of 0-3% [13,14].

. Adapted from: Allaham AH, Estrera AL, Miller CC, Achouh P, Safi HJ. Chylothorax complicating repairs of the descending and thoracoabdominal aorta. Chest. 2006;130(4):1138-42.")
 and corresponding lymphangiogram images (B and D) demonstrating dilated lymphatic channels in the retrocrural spaces and retroperitoneum (solid white arrows).")
, creation of a longitudinal incision along the dorsum of the foot (B), and isolation of a lymphatic duct (C and D).")
 and evaluation of its progression through the lower extremity (B) and pelvis (C) (solid white arrows).")
, continuous fluoroscopic monitoring to access the cisterna chyli (B), and guidewire placement into the thoracic duct (C).")
 (solid white arrows) and an abrupt cut off (B) with massive contrast extravasation (C) (solid white arrows) consistent with thoracic duct injury and leakage.")
 (solid white arrows) and N-butyl cyanoacrylate glue distally (B) (solid white arrows).")