ECR 2015 / C-1536
Revisiting a traditional technique in vascular intervention: Use of self-made wire snares for retrieval of intravascular foreign bodies
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2015
Poster Number:
C-1536
Type:
Scientific Exhibit
Keywords:
Foreign bodies, Technical aspects, Removal, Cost-effectiveness, Catheter venography, Catheter arteriography, Veins / Vena cava, Vascular, Interventional vascular
Authors:
M. Jehangir, A. Rana, E. M. Kiani; Islamabad/PK
DOI:
10.1594/ecr2015/C-1536

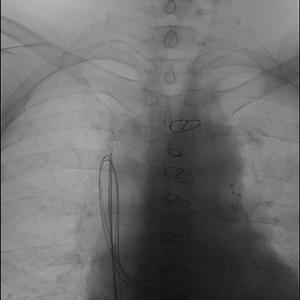
Fig. 2:
47-year-old male with misplaced guide wire lost during central venous access...

Fig. 3:
Loop of self made wire snare advanced just beyond the end of coiled foreign body

Fig. 4:
Ensnared guide wire

Fig. 5:
Ensnared guide wire now slides downwards through inferior vena cava for removal...