ECR 2015 / C-1651
Alkaline-encrusted pyelitis and cystitis: CT and sonography imaging characteristics
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2015
Poster Number:
C-1651
Type:
Educational Exhibit
Keywords:
Digital radiography, Ultrasound, CT, Urinary Tract / Bladder, Kidney, Abdomen, Education, eLearning, Calcifications / Calculi, Infection
Authors:
R. Gil, M. Rengel Ruiz, S. Flores Casaperalta, M. Rausell Félix, M. J. Moreno Gomez, G. Silla, C. Parrilla Muñoz; Valencia/ES
DOI:
10.1594/ecr2015/C-1651

Fig. 1:
Unenhanced CT scan shows bilateral hydronephrosis and thickening of urothelial...
 in a patient with bilateral nephrostomy (yellow arrow). References: Servicio de Radiodiagnóstico, Hospital Clínico Universitario de Valencia. Spain")
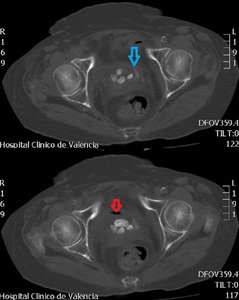
Fig. 2:
Calcifications of the calyces of two kidneys (red arrow) in a patient with...
. References: Servicio de Radiodiagnóstico, Hospital Clínico Universitario de Valencia. Spain")
Fig. 3:
Calcifications of the calyces of two kidneys in a patient with bilateral...

Fig. 4:
Right kidney. Thin and regular calcifications that superficially covers...

Fig. 5:
Left kidney sonogram. Another patient with hyperechogenic structures in calices...

Fig. 6:
Abdominal radiograph shows bilateral urothelial wall thin an regular...
 associated with free stones in a patient with bladder-vaginal fistula (red arrow shows air bubble). References: Servicio de Radiodiagnóstico, Hospital Clínico Universitario de Valencia. Spain")
Fig. 7:
Unenhanced CT scan shows thickening of bladder wall with encrusted...

Fig. 8:
Sonogram of bladder reveals a superficial and hyperechogenic layer with...

Fig. 9:
Longitudinal sonogram of bladder shows hyperechogenic structures with acoustic...
 Unenhanced CT scan shows thickening of bladder wall with encrusted calcification. References: Servicio de Radiodiagnóstico, Hospital Clínico Universitario de Valencia. Spain")
Fig. 10:
a) Unenhanced CT scan shows thickening of bladder wall with encrusted...
 Abdominal radigraphy pre urination where we can see an urothelial wall encrustation in the bladder in a patient with schistosomiasis.
b) Abdominal radigraphy post urination where we see an empty bladder. References: Servicio de Radiodiagnóstico. Hospital Clínico Universitario de Valencia. Spain.")
Fig. 11:
a) Abdominal radigraphy pre urination where we can see an urothelial wall...
 Abdominal radigraphy pre urination where we can see an urothelial wall encrustation in the bladder in a patient with schistosomiasis.
b) Abdominal radigraphy post urination where we see an empty bladder. References: Servicio de Radiodiagnóstico. Hospital Clínico Universitario de Valencia. Spain.")
Fig. 12:
a) Abdominal radigraphy pre urination where we can see an urothelial wall...

Fig. 13:
Curvilinear calcification in left vesicoureteral junction in a patient with...