Achiles tendinopathy (AT):
Achilles tendinopathy represents tendon degeneration without inflammation.
This typically occurs in the midsubstance of the tendon (2-6 cm from the insertion),
where it is theorised there is a zone of relative hypovascularity[1].
A variant also preferentially affects the insertional part of the tendon.
The lifetime incidence in the general population is 7/100000 and higher in athletes,
and up to 29% of runners may be affected[1].
Athletes of all levels are affected,
typically running and jumping sports.
Various medical conditions can predispose to tendinopathy such as connective tissue disorders.
Prescription drugs such as fluoroquinolone and corticosteroids also increase susceptibility to tendinopathy[1].
Patients present with pain and stiffness in midsubstance/insertion of Achilles tendon. Pain worse with activity and relieved by rest.
On examination pain on palpation,
crepitus on motion,
and absence of clinical findings consistent with Achilles rupture may be found.
Histologically tendinopathy is characterised by tendon enlargement neovascularity and neoneural ingress into the tendon.
These changes underlie the pain associated with the condition.
Because these new vessels grown in from outside the tendon,
microadhesions form[2-4].
Imaging findings reflect these histological changes.
On ultrasound:
- tendon thickening
- focal bulge may be seen
- echopoor change
- hypervascularity on Doppler
- structural disorganisation

Fig. 5: Diffuse tendon enlargement with hypoechoic areas and disruption of normal fibriillar pattern consistent with Achilles tendinopathy
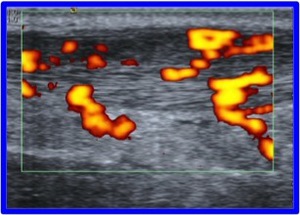
Fig. 6: Power Doppler demonstrates diffuse abnormal hypervascularity of the midsubstance of the Achilles tendon. Note the mid-tendon bulge
References: otto chan
Similar changes occur near the insertion in the insertional variant.
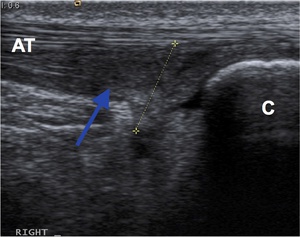
Fig. 8: Longitudinal ultrasound shows normal midsubstance Achilles tendon (AT) and the tendinopathic insertional component (blue arrow) near the calcaneum (C) with ill-defined hypoechoic change and loss of normal fibrillary pattern.
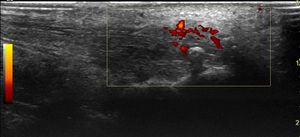
Fig. 9: Longitudinal ultrasound of a different patient again shows similar tendinopathic changes of the insertional component, including evidence of calcium deposition. Power Doppler examination reveals increased vascularity.
On MRI:
- focal bulge
- diffuse high signal
- intrasubstance high signal

Fig. 7: Sagittal fat-supressed proton density MRI shows increased signal within the distal Achilles tendon (arrow), which is also enlarged, near the calcaneum.
Treatments for AT[5]
Conservative - Avoid activities that worsen pain,
eccentric plantar flexion protocol,
Shockwave therapy.
Interventions - Injections of local anaesthetic + steroid,
dry needling,
platelet rich plasma (PRP),
High volume image guided injection (HVIGI),
Prolotherapy.
Little evidence for anything other than eccentrics[5].
HVIGI for Achilles tendinopathy[6]
Mechanisms of HVIGI:
HVIGI acts in myriad ways to treat tendinopathy-
- Breaks adhesions
- Stripping effect - disrupts vessels / nerves / periosteum
- Stretch
- Compression
- Addresses pain and promotes healing
- Cytotoxic / “cell effect”
Each component of the injectate acts differently to effect these actions:
- Volume/saline - disrupts adhesions/stripping/stretch
- Marcaine - exerts neurotoxic effect,
pain relief
- Steroid - stops formation of adhesions/promotes healing
All these act synergistically in conjunction with physiotherapy,
which prevents recurrence.
Equipment required:
- Skin cleaning agent
- Needles of varying sizes
- Luer lock syringes
- High pressure connection tubing
- 40 mls normal saline
- 10 mls 0.5 % marcaine
- 25 mgs hydrocortisone
- High frequency linear ultrasound probe
- Assistant
- Note no local anaesthetic or sedation required.

Fig. 10: Equipment required for HVIGI (L->R):
Chlorohexidine for skin preparation, marcain, corticosteroid, saline, luer lock syringe, connector tubing, needles (ultrasound not shown).
References: otto chan
Technique:
- Obtain consent
- Patient in supine position with hip/foot externally rotated
- Clean skin
- Select needle size
- Connect needle to high pressure connection tube
- Connect tubing to luer lock syringe
- US guided percutaneous access into appropriate site,
anterior to Achilles tendon and posterior to Kager's fat pad.
The ultrasound probe should be positioned axially for this step.
- Inject.
Having gained access into the appropriate site with the probe located axially,
the probe should be rotated through 90 degrees to visualise the tendon longintudinally during injection.
Initally inject marcaine and steroid mixture then 4 x 10mls of normal saline to provide maximal distension.
- Video / image real time
- Post-injection images
- Physiotherapy protocol

Fig. 11: Positioning for HVIGI procedure: percutaneous access under US guidance initially in axial plane.

Fig. 12: Intra-procedural photograph. The initial US-guided injection of local anaesthetic and steroid is being injected anterior to the Achilles tendon, to be followed by the four syringes of saline (on the couch)
References: otto chan

Fig. 13: Axial ultrasound image shows the needle located in between the anterior aspect of the Achilles tendon and Kager's fat pad, suitable to commence HVIGI.
References: otto chan

Fig. 14: After placing the needle correctly in the axial plane the probe should be rotated through 90 degrees to image the tendon longitudinally. The space between the Achilles and Kager's fat pad should be injected under direct visualisation. Images show appearences before, mid procedure and after full HVIGI respectively with arrows showing injectate in situ.
References: otto chan
Fig. 15: Video showing longitudinal ultrasound of HVIGI in between the abnormal enlarged tendinopathic Achilles tendon and Hoffa's fat pad. Note the massive distension of the space
References: otto chan
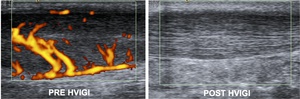
Fig. 16: Power Doppler longitudinal ultrasound images of the Achilles tendon taken before and 2 weeks after HVIGI. Pre image shows a thickened tendon with marked hypervascularity. Post image shows reduction in tendon thickness and no vascularity.
References: otto chan
Rehabilitation programme:
3 days - rest
3 days - start eccentrics for life
3 days - swim,
cycle,
cross-train or row
3 days - gentle training
Sport - 10-12 days after HVIGI
Fitness program - 50% of time off
Partial Achilles tendon tears
Partial tears may occur in both athletes and sedentary individuals,
and often in those with pre-existing AT.
Patient report pain in the Achilles region and reduced function and there is likley to be localised tenderness on examination.
Imaging of partial tears
Ultrasound - Incomplete hypoechoic disruption of fascicular structure & asymmetrical focal tendon enlargement
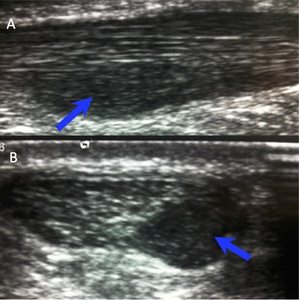
Fig. 19: Longitudinal (A) and axial (B) ultrasound demonstrate focal hypoechoic Achilles tendon enarlgement consistent with partial tear.
References: otto chan
MRI – high signal area (T2/STIR) as above.
Treatment of partial tears
-Image guided prolotherapy and immobilisation in boot for 4-6 weeks
Prolotherapy involves combining a solution of 50% dextrose and 0.5% marcaine at 50:50 dilution to create a solution of 25% dextrose in 0.5% marcaine.
Mix a volume of 3mls in a syringe and inject 0.3 ml aliquots into the area of interest (usually 3-4 aliquots are sufficient)
-Surgery is not an option.
Intratendinous Achilles tendon tears (ITT)
Intratendinous tears are a subset of partial Achilles tears.
They occur in elite athletes,
and are more common in males than females.
Patients often have a background of Achilles tendinopathy.
Those who get ITTs report a sudden onset localised pain in the Achilles region.
They remain able to train but are unable to perform maximal loading (ie sprint).
On examination there are signs of AT,
along with localised pain on palpation.
Complete rupture should be excluded.
Imaging of ITTs
Ultrasound – ovoid/linear hypoechoic area situated centrally in the tendon or extending to,
but not through,
the tendon periphery.
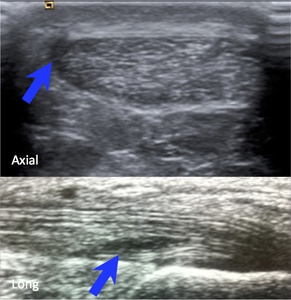
Fig. 17: Axial and longitundinal ultrasounds demonstrate focal hypoechoic areas(curvilinear and linear respectively) confined to the Achiles tendon (blue arrows) consistent with ITT.
References: otto chan
MRI – high signal intratendinous area (T1,
FST2/STIR) as above.

Fig. 18: Axial T2-weighted MRI shows focal high signal in the lateral aspect of the Achilles tendon without change in tendon contour consist with ITT.
References: otto chan
Features of AT will often also be found.
Treatment of ITTs
Image guided prolotherapy (as above) and immobilisation in boot for 4-6 weeks.
Plantaris injury/tendinopathy
Plantaris is a common vestigial muscle (7 – 20% of population) – seen in over 90% on ultrasound.
Originates from posterosuperior aspect of lateral femoral condyle and runs between soleus and gastrocneumius,
crossing obliquely from lateral to medial.
The plantaris tendon runs along the medial border of Achilles tendon and has a variable insertion,
often inserts with it into the posterior calcaneus,
but can occassionally fuse with it more proximally.
Planataris disorders typically occur in athletes of all levels.
They will usually report a background history of AT symptoms.
Injuries will present with an acute history.
Patients report pain on medial side of the Achilles.
On examination there is tenderness on medial side of Achilles and often clinical features of AT.
Importantly there is no impairment of ankle function.
Imaging features of plantaris injury/tendinopathy
Ultrasound – Enlarged,
hypoechoic and blurred plantaris tendon,
usually distal to gastrocnemius and medial to Achilles tendon
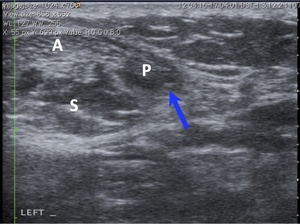
Fig. 21: Axial ultrasound shows abnormally thickened, hypoechoic and irregular plantaris tendon (P and blue arrow). Close relationships to Achilles tendon (A) and soleus (S) are shown.
References: otto chan
MRI – Thickened plantaris with surrounding high signal (T2/STIR)
Treatment of plantaris injury/tendinopathy
Conservative - rest,
eccentric protocol
Image guided intervention - Inject PRP,
prolotherpy and boot, HVIGI
Fascia cruris tears [7]
The fascia cruris is a thin layer of connective tissue that encircles the structures of the posterior calf and is a load bearing structure.
It is closely related to Achilles tendon and continuous with its paratenon.
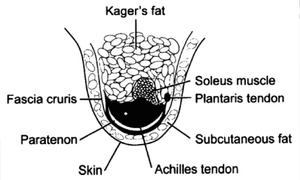
Fig. 22: Axial schematic shows the relationship of the FC to the paratenon and Achilles tendon, surrounding them on the medial, dorsal and lateral sides.
References: otto chan
It acts as a pulley during powerful inversion and eversion of the ankle.
Because the FC invests both sides of the Achilles tendon,
injuries to either the medial or lateral aspect can occur,
and therefore may give rise to symptoms on either side accordingly.
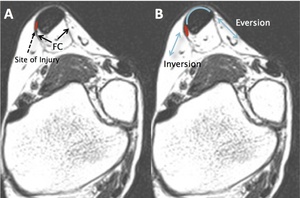
Fig. 23: Axial MRI sections demonstrate:
A - the fascia cruris (FC) encircling the Achilles tendon;
B - motion of fascia cruris during inversion and eversion of the ankle and the site of injury (red) when the fascia cruris tears during powerful movements of the ankle. Injuries may either occur on the medial or lateral sides.
References: otto chan
Injuries to the FC usually occur in elite athletes,
especialy those with with overpronation.
Aetiologically,
they are caused by unusual or excessively strenuous activity.
Sufferers typically experience a sensation of calf tightness over the preceding days or weeks and then a rapid onset of pain in the Achilles region during activity[7].
On examination there is a mild swelling over the mid to upper portion of the Achilles tendon,
tender to the touch,
medially or laterally.
A palpable tightness is noted in the soleus and gastrocnemius.
Imaging of FC tears:
Ultrasound - hypoechoic area (often globular or V-shaped) adjacent but separate to the Achilles,
either medial or lateral.
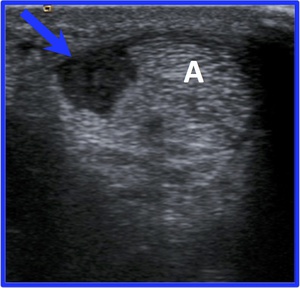
Fig. 24: Oblique axial ultrasound shows a large globular hypoechoic area in the lateral FC (blue arrow) clearly distinct from the Achilles tendon (A), consistent with FC tear.
References: otto chan
MRI – subtle (T1/fat sat T2/STIR) high signal area adjacent to Achilles,
either medial or lateral.
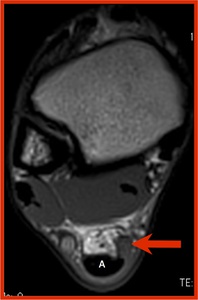
Fig. 25: Axial T2-weighted MRI shows globular area of intermediate signal within medial FC consistent with FC tear. Again the normal Achilles tendon (A) is clearly seen to be distinct from the FC tear. The normal thin FC is seen on the anterolateral side of the Achilles tendon.
References: otto chan
Treatment of FC tears :
- Rest
- Eccentrics as per AT
- Image guided prolotherapy (25% dextrose/0.5% marcaine protocol as above) into fascia cruris
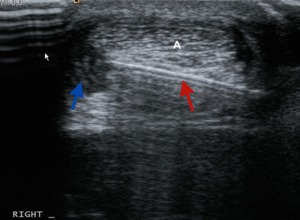
Fig. 26: Axial ultrasound shows needle (red arrow) placed with tip in FC tear (blue arrow) prior to injection of prolotherapy agent
References: otto chan
Fig. 27: Axial ultrasound shows percutaneous access into the globular FC tear (distinct from Achilles tendon) and start of injection of prolotherapy
References: otto chan
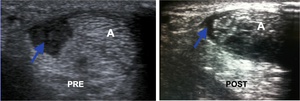
Fig. 28: Axial ultrasound images show large irregular ovoid hypoechoic tear of lateral FC (blue arrow), clearly distinct from the Achilles tendon (A). Follow up ultrasound after prolotherapy shows marked resolution of the tear (blue arrow).
References: otto chan
Acute muscle injury:
Athletes of all levels can develop acute muscle injury.
The gastrocneumius and soleus are intimately related to the Achilles tendon.
Muscle injuries may occur due to excessive tensiles forces (eg sprinters) or contusion (eg contact or combat sports).
Where due to tensile forces,
they typically occur during the eccentric phase.
Patients present with sudden onset pain and disability,
but this depends on the degree of injury.
On examination there is soft tissue swelling and bruising,
pain in posterior calf,
impairment of plantar flexion.
Imaging of acute calf muscle injuries [8]:
Grade 0 – Normal appearance on MRI and US,
but with clinical Dx of muscle injury
Grade I – change in echogenicity and blurring of fibres with feathery appearance
Grade II – Loss of feathery appearance and discontinuity of some fibres
Grade III – Complete disruption and separation of fibres,
usually at musculotendinous junction.
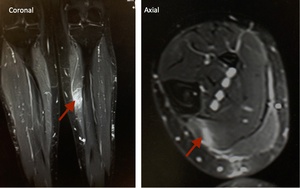
Fig. 29: Coronal and axial STIR MRI show linear focal high signal within the medial soleus consistent with acute muscle tear
References: otto chan
Treatment of acute muscle injuries:
Conservative
- Rest,
Ice,
Compression,
Elevation
- Hyperbaric oxygen
- Physiotherapy
Image guided intervention
- PRP injection
- Injecton with Trameel/Activigin
- Trigger point injections

:
Chlorohexidine for skin preparation, marcain, corticosteroid, saline, luer lock syringe, connector tubing, needles (ultrasound not shown). References: otto chan")

 References: otto chan")



, clearly distinct from the Achilles tendon (A). Follow up ultrasound after prolotherapy shows marked resolution of the tear (blue arrow). References: otto chan")
 placed with tip in FC tear (blue arrow) prior to injection of prolotherapy agent References: otto chan")
 and axial (B) ultrasound demonstrate focal hypoechoic Achilles tendon enarlgement consistent with partial tear. References: otto chan")
 confined to the Achiles tendon (blue arrows) consistent with ITT. References: otto chan")

")
. Close relationships to Achilles tendon (A) and soleus (S) are shown. References: otto chan")
