The pathology involving cranial nerves comprises trauma,
inflammation (infection,
autoinmune,
autoimmune-related diseases),
primary or secondary tumors,
vascular and idiopathic causes.
Also,
it can be divided according to the segment of the nerve affected from the central nuclei in the brainstem to the peripheral branches. It is worth mentioning that apart from the intrinsic injuries,
all cranial nerves are exposed to extrinsic lesions such as compression by intracranial neoplasms or aneurysms.
1.
TRAUMA
Cranial nerve injury in head trauma is in the region of 5-23%.
Injury to the cranial nerves can occur not only secondary to head trauma but also as a sequel to surgical procedures.
Trauma can affect a single or various craneal nerves.
Overall,
the mechanism and symptoms are summarized in the following tables:
Fig. 4
Fig. 5
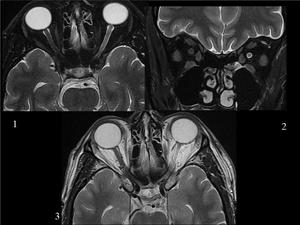
Fig. 6: TRAUMA. This patient refered monocular visual loss after head trauma. These images obtained 10 months after the injury show a thin and hyperintense second left cranial nerve compared with the right one. Axial fat-saturated T2 weighted image(WI)(1)fat-saturated coronal T2 (2) and axial T2 WI (3).
2.
INFLAMMATION
It can be caused by infection,
autoinmune,
autoimmune-related diseases or idiopathic causes.
The main nerves and pathologies included in this category are the following:
BELL PALSY
Nowadays,
it is thought to be due to a reactivation of a latent herpetic infection of the geniculate ganglion.
The typical clinical presentation is acute peripheral VII cranial nerve paralysis.
There are two main patterns of enhancement: uniform contiguous or only in IAC fundus in conjunction with temporal segments.
It is worth mentioning that normal intratemporal facial nerve enhances,
however to a lesser degree than in Bell palsy,
so enhancement should be compared to the other side.
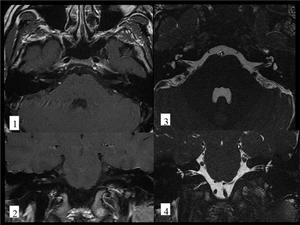
Fig. 7: BELL'S PALSY. 28 year-old man with acute right facial palsy. He recovered completely few days later. Axial(1) and coronal(2) postcontrast T1 images show subtle enhancement of the right facial nerve in the fundus of the internal auditory canal .Axial(3) and coronal(4)FIESTA images show no abnormal findings.
RAMSAY-HUNT SYNDROME
It is considered a reactivation of the Varicella Zoster Virus lodged dormant in the geniculate ganglion.
Both VII and VIII are involved,
mainly in the fundus of the IAC,
intratemporal facial nerve and membranous labyrinth.
After a few days of ear pain,
the patient suffers from facial palsy and sensorineural hearing loss.
There are usually ear vesicles and inflammation in the external ear.
MENINGITIS
Tuberculous meningitis
There are two manifestations of tuberculosis in central nervous system(CNS): tuberculous meningitis,
more frequent,
and parenchymal tuberculosis (tuberculomas).
Both are usually the result of hematogenous spread.
Meningitis is characterized by abnormal meningeal enhancement,
more pronounced in the basal cisterns .
The differential diagnosis includes other microrganisms,
noninfectious inflammatory meningitis or neoplastic meningitis.
As for tuberculomas,
at CT appear as round masses with homogeneous or ring enhancement and irregular walls of varying thickness.
NEUROSARCOID
The cranial nerve involvement in sarcoidosis can be due to leptomeningeal disease or brain tissue granulomas infiltration along perivascular spaces.
The radiological main finding is cranial nerve enhancement on MRI.
At autopsy,
CNS sarcoid involvement has been reported to be present up to 25% of patients,
whereas only 10% of patients show symptoms.
The prognosis ranges from a self-limiting process to a progressive course.
OPTIC NEURITIS
It is believed to be an autoimmune process.
The most common symptoms are acute loss of visual acuity and eye pain.
Approximately,
half of the patients with optic neuritis will develop multiple sclerosis.
Optic nerve is a preferent site in desmielinitating lesions.
The differential diagnosis includes ischemic optic neuropathy,
specially in older patients.
The MR findings are T2 hyperintensity and enhancement of the optic nerve,
which is normal or slightly enlarged.
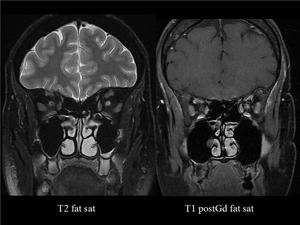
Fig. 8: OPTIC NEURITIS. The left optic nerve shows increased signal on T2WI and enhances in T1 postcontrast WI, both with fat saturation.
3.
TUMORS
As mentioned above,
the olfactory and optic nerves are not true nerves but an extension of the brain,
that´s why they are affected by tumors such as gliomas and meningiomas in contrast to III-XII neves that can develop schwannomas.
SCHWANNOMAS
A schwannoma is a slowly growing benign tumor that arises from Schwann cells,
that in conjunction with a collagenous matrix create the nerve sheath.
Schwannomas may arise in III-XII cranial nerves,
yet,
it remains unclear its preference for VIII nerve,
specially its vestibular division,
in fact,
schwannomas arising in the VIII cranial nerve represent approximately 95% of all intracranial schwannomas .
Its malignant counterpart is extremely rare and generally associated with neurofibromatosis 1.
VESTIBULAR SCHWANNOMA
As mentioned above,
schwannomas arising in the VIII cranial nerve are much more often than from any other cranial nerve.
Its radiological features consist of a mass in the internal auditory canal with possible extension to cerebellopontine angle (IAC-CPA); if so,
the morphology is of an “ice-cream on cone”.
On MRI,
it is hyperintense on FLAIR,
and on T1 weigthed images when hemorrhage is present.
After intravenous contrast,
it enhances avidly.
Besides,
schwannomas can show cysts.
Bilateral acoustic schwannomas are present in patients with neurofibromatosis 2 in approximately 96%.
Schwannomas in NF2 usually appear before 21 years of age and are more prone to infiltration of facial and cochlear nerves.
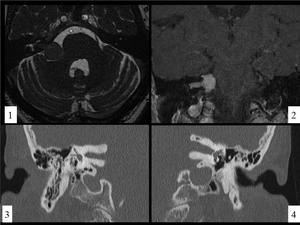
Fig. 9: VESTIBULAR SCHWANNOMA.Case A. There is a mass in the Cerebellopontine angle-internal auditory canal (CPA-IAC) cistern with the typical "ice-cream on cone" shape (image 1), that enhances on coronal postcontrast T1 image. Case B. CT images show an asymmetry in the IAC, being wider the left one due to an expanding mass(not shown) consistent with a vestibular schwannoma.
TRIGEMINAL SCHWANNOMA
Schwannomas from the fifth nerve are the second in order of frequency.
Intradurally,
the trigeminal schwannomas originate from the cisternal segment or Meckel’s cave,
while extradurally,
from the gasserian ganglion in the middle cranial fossa.
Compared with acoustic schwannomas,
trigeminal schwannomas are more likely to contain cystic components.
Their CT findings are an iso slightly hypodense nerve enlargment that enhances in homogeneous or heterogeneous way.
Their MR features are similar to those of vestibular schwannomas.
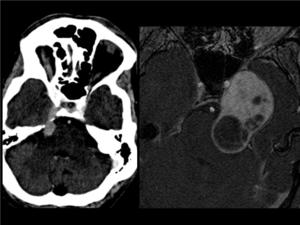
Fig. 10: TRIGEMINAL SCHWANNOMA.CASE a. CT image shows an enlarged enhancing right trigeminal nerve in its cisternal and cranial segments. CASE b. On the axial postcontrast T1WI there is an enhancing mass with cystic components (more frequent than in vestibular schwannomas), probably arising in the Meckel's cave with extension to the prepontine cistern and mass effect on the pons.
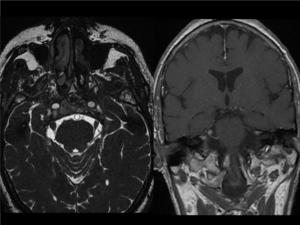
Fig. 11: TRIGEMINAL SCWANNOMA. There is a thickening of the right trigeminal nerve in its cisternal segment (axial FIESTA). It enhances after intravenous contrast (coronal T1 postcontrast image).
FACIAL NERVE SCHWANNOMA
It may arise from any segment of the facial nerve; when arising in the IAC-CPA is depicted as a mass with those characteristic of vestibular schwannoma,
which makes it difficult to distinguish from vestibular schwannomas. If a labyrinthine canal “tail” is present,it can be helpful to differentiate them.
ESTHESIONEUROBLASTOMA
This tumor is located at the cribiform plate and extends to anterior cranial fossa and to the nasal cavity in a dumbbell-like morphology.
Esthesioneuroblastoma shows intense enhancement,
hypointense to intermediate signal intensity on T1WI,
intermediate to hyperintense in T2WI and can have areas of cystic degeneration.
OPTIC GLIOMA
Optic nerve gliomas in children are generally low grade astrocytomas,
while in adults are usually high-grade gliomas.
They are associated with neurofibromatosis 1,
specially when bilateral.
Its imaging appearance is optic nerve thickening with isointense to white matter signal on T1 and T2 weighted images. It also can show cysts.
The enhancement is variable,
from none to intense.
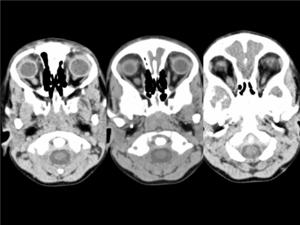
Fig. 12: OPTIC GLIOMA in a 4 year-old boy. Axial CT images demonstrates a thickened left optic nerve in its intraorbital segment.
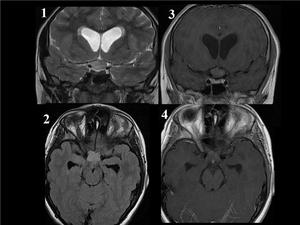
Fig. 13: OPTIC GLIOMA in a 12 year-old boy. Coronal T2 WI (image 1) and axial FLAIR image (image 2) show diffuse enlargement of the chiasma. Coronal and axial postcontrast T1WI (images 3,4)demonstrate minimal enhancement of the chiasma. Besides, it causes third ventricular compression and acute hydrocephalus.
BRAINSTEM GLIOMA
Brainstem glioma usually arises in children and adolescents,
being rare in adults.
It comprises well-defined focal and diffuse infiltrative gliomas,
therefore its signal intensity and enhancement after intravenous contrast are variable.
Distorsion and enlargement of the pons (suggested by blurred prepontine cistern or wavy anterior margin in sagital plane) can be present,
but not always.
Cysts are an infrequent finding.
Among the clinical presentation,
multiple cranial nerve palsies are found.
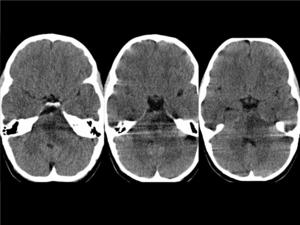
Fig. 14: BRAINSTEM GLIOMA(Diffuse pontine glioma)in a 5 year-old girl with gait disturbance. The consecutive CT images show an ill-defined hypoattenuating mass in the pons which represents a grade IV glioma.
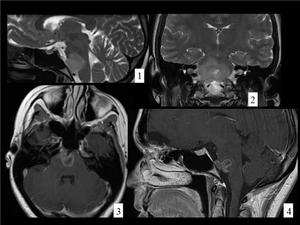
Fig. 15: BRAINSTEM GLIOMA(glioblastoma multiforme in a young adult. Sagital and coronal T2WI (images 1,2) demonstrate an hyperintense mass that expands the pons and surrounds the basilar artery. In the postcontrast T1 images (axial and sagital, images 3,4) the mass enhances in a ring-like fashion. Enhancement at the initial diagnosis indicates poor prognosis.
CEREBRAL METASTASIS
Intraaxial metastasis,
when located at the brainstem,
can produce cranial nerves symtoms due to the injury to their nuclei .
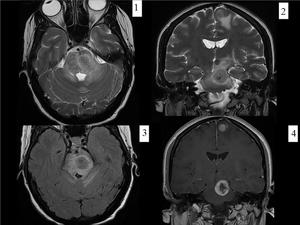
Fig. 16: BRAINSTEM METASTASIS. Woman with history of breast cancer who came to emergency room for perioral hypesthesia (trigeminal territory). There is an intraaxial mass in the left side of mesencephalon and pons which expands the mesencepalon and partially obliterates the perimesencephalic and interpeduncular cisterns. It is surrounded by vasogenic edema that extends to the left cerebral peduncle and middle cerebellar peduncles. These findings are consistent with metastasis.The lesion has hypointense center and hyperintense rim on T2WI (axial T2WI-image 1-, coronal T2WI-image 2-, axial FLAIR-image3) and enhances peripherally (postcontrast coronal T1 image).
CARCINOMATOUS MENINGITIS
The improved survival of cancer patients,
increased knowledge among the clinicians,
and the diagnosis role of MR imaging have contributed to a recently increased in the diagnosis of carcinomatous meningitis .
Metastatic involvement of the leptomeninges is the result of the spread of malignant cells through cerebrospinal fluid.
The most commonly involved tumors are breast,
lung,
melanoma,
non-Hodgkin lymphoma and primary CNS tumors.
MRI findings are linear and nodular enhancement of sulci,
cisterns and ventricles at contrast material–enhanced images.
Associated effacement,
hydrocephalus and cranial nerve enhancement can also be seen.
On FLAIR images increased signal within sulci is usually present.
The diagnosis is confirmed by the presence of malignant cells in cerebrospinal fluid.
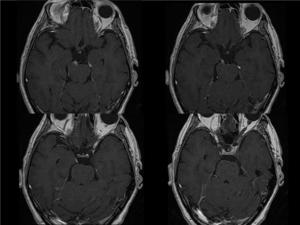
Fig. 17: CARCINOMATOUS MENINGITIS in a patient diagnosed of pleural/rib sarcoma(1)Axial postcontrast T1 images show right third cranial nerve enhancement, since its origin in the brainstem to the cavernous sinus.
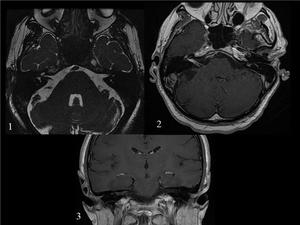
Fig. 18: CARCINOMATOUS MENINGITIS in a patient diagnosed of pleural/rib sarcoma(1)Axial FIESTA image shows subtle thickening of the VII-VIII cranial nerves in the internal auditory canal and extension to the cochlea. The nerves enhance after intravenous contrast injection.Axial (2) and coronal (3) postcontrast T1 images.
PERINEURAL SPREAD
Perineural spread is defined as extension of head and neck tumors along large nerves.
The most common nerves used as routes of tumor spread are the fifth branches and the seventh cranial nerve.
MRI is superior to CT for detecting perineural spread,
which is shown as an enlarged enhancing nerve.
Other signs are: smoothly widened foramina and canals and abnormal soft tissue density at foramina.
The main tumors involved in perineural spread are adenoid cysitic carcinoma,
sqamous cell carinoma,
melanoma and Non-Hodgkin lympoma.
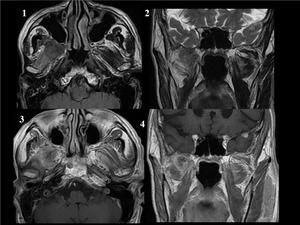
Fig. 19: PERINEURAL SPREAD. There is a mass in the right masticator space arising in the pterigoid muscles. The mass has intermediate T1 and T2 signal and enhances after intravenous contrast. The pterigoid muscles show T2, FLAIR hyperintensity and enhance in contrast to the contralateral muscles. These findings are consistent with indirect signs of perineural infiltration (V3) and implies a recurrence of the malignant parotid neoplasm.
4.
VASCULAR CAUSES
INFARCT/HEMORRHAGE
An acute brainstem stroke,
when affecting cranial nerve nuclei,
can cause isolated or predominant cranial nerve palsy.
Moreover,
hemorrage in the same locations can produce the same symptoms.
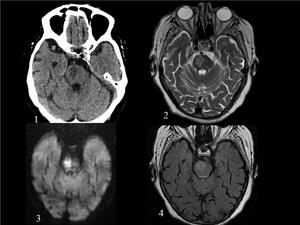
Fig. 20: ACUTE BRAINSTEM STROKE. The patient suffered from acute right central facial paralysis and left hemibody weakness.(1)axial ct image shows a hypoattenuating lesion on the left side of the pons, which is hyperintense on axial T2 WI (2), FLAIR (4) and shows restricted diffusion (4). Findings consistent with acute brainstem stroke.
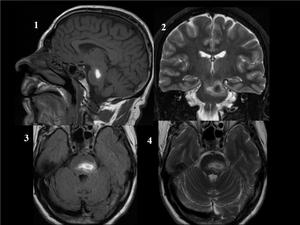
Fig. 21: PONTINE HEMORRHAGE. In the pons, there is an acute/subacute hemorrhage. Sagital T1WI (image 1), axial FLAIR and T2 WI reveal a hyperintense lesion in the pons. On coronal T2 WI, the hyperintense pontine hemorrhage have hypointense center, findings consistent with acute hemorrhage.
ICA DISSECTION
Clinical manifestations range from carotid territory ischemia to head or neck pain,
Horner syndrome and cranial nerve palsy.
The main radiological finding is a narrow eccentric lumen surrounded by a crescent-shaped mural external thickening (corresponding to the wall hematoma,
hyperattenuating at unenhanced CT).
It may be helpful to be familiar with the common dissection sites( a few centimeters after the origin of ICA or below the skull base) in order to differentiate the resembing atherosclerotic thickening from dissection.
Other signs of arterial dissection are an intimal flap and a dissecting aneurysm.
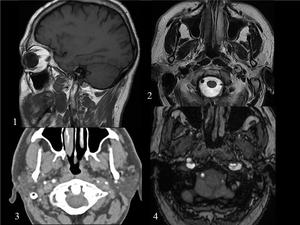
Fig. 22: LEFT INTERNAL CAROTID ARTERY (ICA). 39 year-old man with acute left headache and left hypoglossal nerve paralysis. (1) Sagital T1 image shows an hyperintense hematoma extending along the ICA wall.(2)Axial T2 WI and (3)axial TC angiography image demonstrate narrow eccentric lumen surrounded by a crescent-shaped mural hematoma.(4)3D TOF shows double lumen in the left ICA.
ANEURISM
The third cranial nerve in its cisternal segment travels between the posterior cerebral and superior cerebellar arteries,
as a result,
it is vulnerable to compression by a posterior communicating artery aneurysm.
In fact,
the most frequent cause of an isolated third cranial nerve palsy affecting the pupil is an aneurysm at the internal carotid-posterior communicating artery junction.
Generally,
there is a subsequent aberrant regeneration after an acute third cranial nerve palsy due to trauma or aneurysm.
Berry aneurysms of the AICA are quite rare and can be mistaken for acoustic schwannomas.
VERTEBROBASILAR DOLICHOECTASIA
It is defined as an elongation (any segment of the artery extends lateral to the margin of the clivus/the dorsum sellae or it bifurcates above the plane of the suprasellar cistern) and dilatation (diammeter> 4,5 mm on CT) of the basilar artery.
It has been reported that can cause compressive symptoms of the posterior fossa cranial nerves,
such a hemifacial spasm or paresis or trigeminal neuralgia.
LOOP OF THE AICA
A loop of the anterior inferior cerebellar artery (AICA) has been attributed to cause vertigo.
The AICA describes a loop before giving rise to the auditory artery.
This loop can be situated in the APC cistern,
close or in contact with VII-VIII nerves,
at the porus or in the IAC.
However,
this finding does not imply compressive symptoms.
TRIGEMINAL NEURALGIA
The significance of the vascular loop compressing the trigeminal nerve is unclear due to this finding is present in symptomatic and asymptomatic patients observed incidentally.
SUPERFICIAL (PIAL) SIDEROSIS
It is the result of repeated episodes of subarachnoid hemorrhage.
The VIII nerve is more susceptible to the harmful effects of iron and hemosiderin probably due to its long cisternal segment and the fact that the transition from glial-Scwhann cells occurs near the IAC.
On MRI,
a marked hypointensity on T2 and T2*GRE in the pial,
arachnoid membranes and cranial nerves is shown because of the deposit of iron.
5.
IDIOPATHIC
6.
OTHERS
Lesions arising in base of skull such as chordoma,
chondroma,
chondrosarcoma,
chondromyxoid tumor,
metastasis...or cerebellopontine angle tumors for instance meningiomas can compress the brainstem and so produce cranial nerve symptoms.
Furthermore,
The III,IV,V and VI cranial nerves can be altered by lesions in the region of cavernous sinus or in the superior orbital fissure.
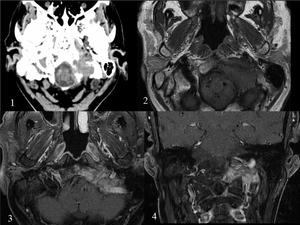
Fig. 23: LUNG METASTASIS in OCCIPITAL BONE with extesion to JUGULAR FORAMEN.The patient presented with jugular foramen or Vernet's syndrome, in other words, paresis of 9th–11th with or without involvement of 12th. There is a soft tissue mass that invades the left condyle and basilar process of the occipital bone, which includes the hypoglossal canal and jugular foramen. Axial CT image (1), pre- and post-contrast axial T1WI (2,3) and postcontrast coronal T1WI(4).
CAVERNOUS SINUS SYNDROME
Cavernous sinus syndrome is defined by multiple cranial neuropathies namely: Horner’s syndrome,
ophthalmoplegia,
chemosis,
proptosis and sensory loss of the first or second divisions of the trigeminal nerve.
The pupil may be affected or spared.
The lesions that involve the cavernous sinus are infectious (cavernous sinus thrombophlebitis,
actinomycosis,
rhinocerebral mucormycosis,
aspergillosis),
noninfectious inflammation (Tolosa-Hunt syndrome ,
inflammatory pseudotumor),
vascular lesions (aneurysm of the internal carotid artery,
carotid–cavernous fistula,
dural arteriovenous fistula) and tumors (direct invasion of pituitary adenomas,
perineural or hematogenous spread metastasis...).
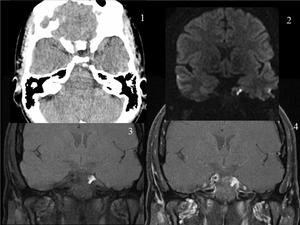
Fig. 24: DERMOID CYST in the cavernous sinus.Patient with sixth cranial nerve palsy. The images demonstrates an extra-axial mass located in the left middle cranial fossa involving the left cavernous sinus. The mass is hypertense on T1, DW and T2 (not shown)images and shows no enhancement.
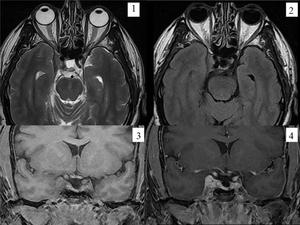
Fig. 25: cavernous sinus meningioma.The MR images demonstrate an extra-axial mass that involve the right cavernous sinus. The mass is T1 isotense and T2 hyperintense with contrast enhancement. Not present in this case, but meningimas usually narrow the cavernous ICA. (axial T2WI-image 1-, axial FLAIR- image2-, pre- and post-contrast coronal T1- images 3,4).



(1)fat-saturated coronal T2 (2) and axial T2 WI (3).")
 and coronal(2) postcontrast T1 images show subtle enhancement of the right facial nerve in the fundus of the internal auditory canal .Axial(3) and coronal(4)FIESTA images show no abnormal findings.")

 cistern with the typical "ice-cream on cone" shape (image 1), that enhances on coronal postcontrast T1 image. Case B. CT images show an asymmetry in the IAC, being wider the left one due to an expanding mass(not shown) consistent with a vestibular schwannoma.")
, probably arising in the Meckel's cave with extension to the prepontine cistern and mass effect on the pons.")
. It enhances after intravenous contrast (coronal T1 postcontrast image).")

 and axial FLAIR image (image 2) show diffuse enlargement of the chiasma. Coronal and axial postcontrast T1WI (images 3,4)demonstrate minimal enhancement of the chiasma. Besides, it causes third ventricular compression and acute hydrocephalus.")
in a 5 year-old girl with gait disturbance. The consecutive CT images show an ill-defined hypoattenuating mass in the pons which represents a grade IV glioma.")
 demonstrate an hyperintense mass that expands the pons and surrounds the basilar artery. In the postcontrast T1 images (axial and sagital, images 3,4) the mass enhances in a ring-like fashion. Enhancement at the initial diagnosis indicates poor prognosis.")
. There is an intraaxial mass in the left side of mesencephalon and pons which expands the mesencepalon and partially obliterates the perimesencephalic and interpeduncular cisterns. It is surrounded by vasogenic edema that extends to the left cerebral peduncle and middle cerebellar peduncles. These findings are consistent with metastasis.The lesion has hypointense center and hyperintense rim on T2WI (axial T2WI-image 1-, coronal T2WI-image 2-, axial FLAIR-image3) and enhances peripherally (postcontrast coronal T1 image).")
Axial postcontrast T1 images show right third cranial nerve enhancement, since its origin in the brainstem to the cavernous sinus.")
Axial FIESTA image shows subtle thickening of the VII-VIII cranial nerves in the internal auditory canal and extension to the cochlea. The nerves enhance after intravenous contrast injection.Axial (2) and coronal (3) postcontrast T1 images.")
 and implies a recurrence of the malignant parotid neoplasm.")
axial ct image shows a hypoattenuating lesion on the left side of the pons, which is hyperintense on axial T2 WI (2), FLAIR (4) and shows restricted diffusion (4). Findings consistent with acute brainstem stroke.")
, axial FLAIR and T2 WI reveal a hyperintense lesion in the pons. On coronal T2 WI, the hyperintense pontine hemorrhage have hypointense center, findings consistent with acute hemorrhage.")
. 39 year-old man with acute left headache and left hypoglossal nerve paralysis. (1) Sagital T1 image shows an hyperintense hematoma extending along the ICA wall.(2)Axial T2 WI and (3)axial TC angiography image demonstrate narrow eccentric lumen surrounded by a crescent-shaped mural hematoma.(4)3D TOF shows double lumen in the left ICA.")
, pre- and post-contrast axial T1WI (2,3) and postcontrast coronal T1WI(4).")
images and shows no enhancement.")
.")