ECR 2015 / C-2352
Unusual muscular diseases: Patterns and Pearls at MR Imaging
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2015
Poster Number:
C-2352
Type:
Educational Exhibit
Keywords:
Oedema, eLearning, Diagnostic procedure, MR, Musculoskeletal soft tissue, Musculoskeletal system, Tissue characterisation
Authors:
D. Armario Bel, D. Durany Lara, M. C. Sanchez Torres ; Badalona/ES
DOI:
10.1594/ecr2015/C-2352
 and axial fat-suppressed T2-weighted (b) images depict a high signal due to edema of regional muscles, especially the vastus medialis (asterisk), and an abnormal bone marrow signal due to edema and devitalized tissue (arrowhead).")
Fig. 1:
10-year-old boy with distal femur osteomyelitis. Coronal STIR (a) and axial...
 and fat-suppressed gadolinium-enhanced T1-weighted image (b) show a subperiostal abscess in the posterior aspect of the distal metaphysis (arrow) and also loculated fluid collections in regional muscles (arrowheads).")
Fig. 2:
10-year-old boy with distal femur osteomyelitis.
Sagital STIR (a) and...
 related to an insufficiency fracture.")
Fig. 3:
Patient with rectal neoplasm treated with radiotherapy.
Axial T2- weighted...
 compatible with osteitis, and also bilateral focal edema of both piriformis muscles (asterisks).")
Fig. 4:
Same patient. Axial T2- weighted fat-suppressed MR image depicts high signal...
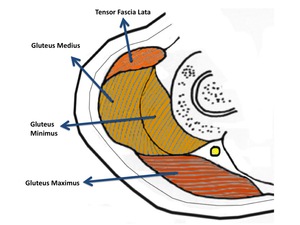
, The Gluteus Medius and Minimus (yellow) and The Gluteus Maximus (red).")
Fig. 5:
Scheme shows the three different compartments of gluteal area: the Tensor...
. Notice the perpendicular line traversing both gluteal maximus muscles (arrows) acquiring a morphology that resemble butterfly wings.")
Fig. 6:
Patient with Crohn disease that required surgery who developed in postoperative...

Fig. 7:
Same patient in coronal fat-suppressed T2-weighted images depict same findgins...
 representing the hypervascularized viable tissue.
This particular morphology resembles "butterfly wings".")
Fig. 8:
Axial and coronal fat-suppressed gadolinium-enhanced T1-weighted images. A...
.")
Fig. 9:
Axial T2- weighted fat-suppressed MR image of both hips shows narrowed...
 and axial (b) T2- weighted fat-suppressed MR image depicts bilateral ischiofemoral narrowing but only focal edema of left quadratus femoris muscle (arrowhead).")
Fig. 10:
26 year-old-woman with left hip pain.
Coronal (a) and axial (b) T2- weighted...
 and coronal (b) T2- weighted fat-suppressed MR images at level of pelvis show abnormal right sacral plexus with high signal intensity (arrowheads), consistent with acute-to-subacute diabetic neuropathy.")
Fig. 11:
41-year-old man with known type 2 diabetes mellitus who presented with left low...
 and coronal (b) T2- weighted fat-suppressed MR images at level of ischiatic region shows abnormally hyperintense cyatic (long arrow). Findings diffusely involve the sciatic nerve.")
Fig. 12:
Axial (a) and coronal (b) T2- weighted fat-suppressed MR images at level of...
 and spinal nerve (long arrow). Note also increased enhancement of left paravertebral muscles (asterisks).")
Fig. 13:
Axial fat-suppressed gadolinium-enhanced T1-weigted images through pelvis show...
 and coronal (c) T1-weighted images show fatty replacement of posterior compartments muscles of both legs, being more severe in right side (arrows).
Axial fast spin-echo T2-weighted image with fat suppression shows diffuse increased signal notably within posterior compartment muscles, specially gastrocnemius and soleus (asterisks). Note also the bulky aspect due to edema in left soleus muscle. There is sparing of the anterior compartments.")
Fig. 14:
64 year-old-man with log-term type II diabetis mellitus.
Axial T1 (a) and...
. This edema pattern is secondary to increased water content and inflammatory changes that accompany the infarction. Subcutaneous and perifascial edema are present.
b, c: Coronal fat suppressed gadolinium-enhanced T1-weighted images show diffuse and heterogeneous enhancement of affected muscles with focal non-enhancing areas, which may represent ischemic myonecrosis (arrows).")
Fig. 15:
A 59-year-old man with history of insulin dependent diabetes mellitus with one...
. Some small nodular lesions are also seen in gluteal muscle (arrowhead).
b: Axial fat-suppressed gadolinium-enhanced T1-weigted image confirm rounded lesions in gluteal muscles with slight enhancement compatible with metastasis (arrowheads).")
Fig. 16:
. Patient with primary pulmonary lymphoma and severe pain and swelling in his...
.
b: Axial fat-suppressed gadolinium-enhanced T1-weigted image also show rounded and enhancing lesions in left semimembranous and right adductor magnus muscles, also compatible with metastasis (arrowhead).")
Fig. 17:
Same patient as previous image.
a: Coronal STIR: diffuse high signal within...

Fig. 18:
8-year-old girl with EEII anesthesia and diffuse muscle atrophy secondary to...
 and T2- weighted fat-suppressed (b) images show a heterogeneous isointense mass within lateral gastrocnemius (asterisks) with a high signal component in T1 and low in T2 FS (arrows) compatible with fat. Fluid-fluid levels are also seen on T2 (asterisks). These MRI imaging findings are pathognomonic of hemangioma.")
Fig. 19:
45 year-old-man with palpable mass in right calf.
Axial T1 (a) and T2-...
. Notice also the small nodular images within the cyst with high signal on T1 and low signal on T2 FS (red asterisks), consistent with fat. This special feature may be helpful in the differential diagnosis of intramuscular cystic lesions.")
Fig. 20:
67-year-old man with psoriatic arthritis treated with anti-TNF who developed a...
, fat-suppressed T1 (b) and fat-suppressed T2 (c) -weighted images depict daughter cysts attached to the germinal layer (arrowheads) as well as the fatty nodules within the cysts (red asterisks).")
Fig. 21:
Same patient as before.
Axial T1 (a), fat-suppressed T1 (b) and fat-suppressed...
 show focal muscle edema involving proximal right rectus femoris muscle (arrow). Note that edema is at junction of muscle and tendon (a). Axial image at slightly more caudal level shows also intramuscular hematoma (asterisk).
Coronal T1 image (c) depicts a fusiform intramuscular hematoma.")
Fig. 22:
Muscle strain with intramuscular hematoma
Axial STIR images (a, b) show...
 and coronal (b) T1-weighted images depict a high signal fusiform lesion within deltoid muscle compatible with lipoma.")
Fig. 23:
Axial (a) and coronal (b) T1-weighted images depict a high signal fusiform...
 and sagital T2-wighted (c) images show a rounded and hyperintense lesion within muscle (red asterisk). Notice the slight and heterogeneous enhancement predominantly at periphery in axial (b) and sagital (d) T1 fat-suppressed gadolinium-enhanced images. Diagnostic biopsy was necessary to reach final diagnosis of myxoma.")
Fig. 24:
Axial T2 fat-suppressed (a) and sagital T2-wighted (c) images show a rounded...
 and T2 fat-suppressed (b) images show a round lesion within brachialis muscle of left arm (arrows), hypointense in both sequences with slight peripheral high signal in T2. Only slight and thin peripheral enhancement was seen after contrast administration (c,d). Although a traumatic antecedent was not known, lesions disappeared 4 months later (not shown), making the diagnostic consistent with nodular fascitis.")
Fig. 25:
Axial T1 (a) and T2 fat-suppressed (b) images show a round lesion within...
 depict an intramuscular mass with isointense signal. Axial and coronal fat suppressed T2- weighted images (b and e) show a hyperintense mass with fine septae (arrowheads) within the lesion. Axial T1-weighted fat-suppressed gadolinium-enhanced image (c) show peripheral and intralesional enhancement (arrows).
Diagnostic biopsy confirmed this new lesion as a metastasis from liposarcoma.")
Fig. 26:
67-year-old woman with known retroperitoneal myxoid liposarcoma and “painful...
 Axial T1-weighted image show a isointense mass within muscles. b, c) Axial and coronal fat-suppressed T2-weighted image show a heterogeneous hyperintense mass within posterior muscles of thigh (long arrows), with central area of higher signal due to necrosis (red asterisk) and a round hypointense image related to blood rests (short arrow). d) Coronal fat-suppressed gadolinium-enhanced T1-weighted image shows enhancement of the tumor and confirms the necrotic central region, which suggests malignancy.")
Fig. 27:
Undifferentiated pleomorphyc sarcoma of thigh.
a) Axial T1-weighted image...