Spinal Involvement
Vertebral abnormalities
In the spine,
dysostosis multiplex includes:
- flattening and elongation of the vertebral bodies (platyspondyly);
- wedge-shaped vertebral bodies with anterior beaking and posterior scalloping,
particularly at the thoracolumbar junction (Fig. 1);
- thoracolumbar kyphosis,
which often results from the combination of an anterior beak and vertebral flattening at T12,
L1 or L2 level (Fig. 1).
The apex of the kyphosis is usually located at the L2 vertebra;
- progressive lumbar gibbus deformity;
- anomalies of the posterior vertebral elements such as hypoplasia of the superior vertebral facets,
which may lead to retrolisthesis of one of the relatively small beak-shaped lumbar vertebrae (Fig. 1) or spondylolisthesis of the vertebrae above a hypoplastic beak-shaped vertebra at the thoracolumbar junction level [1].
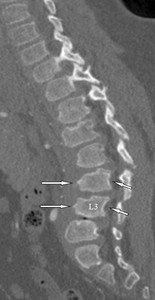
Fig. 1: MPS type II in a 14-year-old boy. Sagittal reformatted CT image of the thoracolumbar spine shows anterior beaking of some vertebral bodies (arrows), thoracolumbar kyphosis, and posterior vertebral scalloping (small arrows). Note retrolisthesis of the beak-shaped L3 vertebra.
References: Leone A et al. (2015) Spinal Involvement in mucopolysaccharidoses: a review. Childs Nerv Syst 31:203-212.
This pattern of vertebral abnormalities evolves over time.
In early childhood,
vertebral bodies have an oval shape,
sometimes with anterior beaking.
In late childhood,
vertebral bodies grow very slowly in height and present anterior beaking,
often associated with posterior scalloping,
particularly at the thoracolumbar junction (Fig. 1).
In adults,
the height of the bodies does not increase from late childhood but the anterior portion of many of the vertebrae ossifies and gives rise to a normal but flattened rectangular configuration on lateral radiographs [5].
However,
there is still an anterior beaking in one or more bodies at the thoracolumbar junction (Fig. 2).
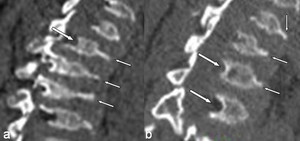
Fig. 2: MPS IV A in a 21-year-old man. (a, b) Sagittal reformatted CT images of the lumbar spine (a) and thoracolumbar junction (b) show some typical thoracolumbar spine changes including platyspondyly, anterior beaking within the midportion of the vertebral bodies (small arrows in a and b) and posterior scalloping of the vertebral bodies (arrows in a and b).
References: Leone A et al. (2015) Spinal Involvement in mucopolysaccharidoses: a review. Childs Nerv Syst 31:203-212.
Skull base anomalies
The pattern of skull base anomalies in MPS includes:
- odontoid dysplasia (e.g.,
dens hypo-or aplasia and/or os odontoideum),
due to incomplete ossification of odontoid process,
which is present in almost all patients with MPS IVA (Fig. 3);
- peri-odontoid soft tissue thickening (Fig. 3);
- laxity of the transverse and alar ligaments.
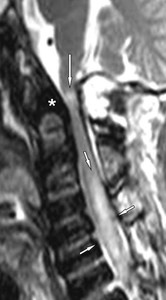
Fig. 3: MPS IVA in a 24-year-old man with neurological manifestations of myelopathy. Sagittal T2-weighted MR image of the cervical spine shows spinal cord compression demonstrated by loss of cerebrospinal fluid and diffuse central spinal canal stenosis at craniocervical junction with a small area of intramedullary increased signal consistent with compressive myelopathy (arrow). Increased signal intensity within the cervical cord from C3 to C7, consistent with edema, is clearly evident as well as mild spinal cord thickening (small arrows). Note odontoid hypoplasia and localized thickening of the surrounding tissue (*).
References: Leone A et al. (2015) Spinal Involvement in mucopolysaccharidoses: a review. Childs Nerv Syst 31:203-212.
Combination of these features can give rise to anterior or vertical atlantoaxial subluxation,
due to excessive independent movement between the anterior arch of the atlas and the dens [6].
GAGs deposits
Another common feature observed in MPS is the accumulation of partly degraded GAGs in the meninges and supporting ligaments,
which contributes to the reduction of the space available for the neural and vascular elements in the spine (Fig. 4).
GAGs deposits are also evident in the peri-odontoid tissue (Fig. 3).
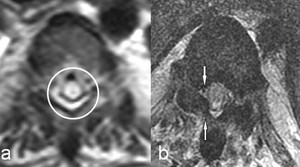
Fig. 4: Same patient as in Fig. 3. a) Transverse T2-weighted MR image passing through T4 vertebra shows spinal cord edema with central gray matter involvement (circle). b) Transverse T1-weighted MR image passing through T8 vertebra shows thickness of the flaval ligament on the right encroaching on the dural sac (small arrows).
References: Leone A et al. (2015) Spinal Involvement in mucopolysaccharidoses: a review. Childs Nerv Syst 31:203-212.
Complications
Common complications in MPS include spinal stenosis,
spinal cord compression and myelopathy,
well evident on magnetic resonance (MR) imaging [1] (Fig. 3, Fig.
4, Fig. 5).

Fig. 5: Same patient as in Fig. 3. Sagittal T2-weighted MR image of the thoracolumbar spine shows multilevel spinal cord compression demonstrated by loss of cerebrospinal fluid and diffuse central spinal canal stenosis (arrows). Increased signal intensity within the thoracolumbar cord, consistent with edema, is clearly evident as well as mild spinal cord thickening (small arrows). Note thoracolumbar kyphosis, platyspondyly, and sternum deformity.
References: Leone A et al. (2015) Spinal Involvement in mucopolysaccharidoses: a review. Childs Nerv Syst 31:203-212.
Spinal cord compression
Spinal cord compression is a common feature in patients with MPS [1,
9-12]; it may involve multiple spinal cord levels,
but usually the thoracolumbar spine (Fig. 5) and,
more frequently,
the craniocervical junction (Fig. 3).
There are two main proposed etiopathologic theories for spinal cord compression.
The first is related to GAGs deposits in the peri-odontoid tissue,
supporting ligaments and meninges [13-16] (Fig. 3, Fig.
4).
The second mechanism is related to vertebral abnormalities,
dysplasia of the odontoid process (Fig. 3),
ligamentous laxity and invagination of the posterior arch of atlas leading to atlantoaxial subluxation and instability [13,
14,
17].
Spinal cord compression can lead to compressive myelopathy.
Spinal stenosis
Spinal stenosis represents a condition in which there is diminished space available for the neural and vascular elements in the spine.
It may involve the central spinal canal (central spinal stenosis) (Fig. 5) and/or the intervertebral foramina and the lateral recesses of the central spinal canal (lateral spinal stenosis) [18].
In MPS,
spinal stenosis is mainly due to focal or multilevel thickening of the connective tissues within the central spinal canal,
particularly of the meninges,
posterior longitudinal ligament,
and flaval ligaments,
due to GAGs deposition [12] (Fig. 3).
Myelopathy
Compressive myelopathy is evident as an area of intramedullary increased signal on T2-weighted images at the level of spinal compression,
due to edema,
ischemia or gliosis/myelomalacia (Fig. 3, Fig. 4, Fig. 5).
However,
this finding does not always correlate with signs and symptoms since,
in most circumstances,
the neurological deficits are usually less severe than suggested by MR imaging [20].
Imaging evaluation
Spinal abnormalities in MPS may be evaluated by imaging modalities such as radiography,
CT and MR imaging [1].
Radiography
Standard radiographic examination represents the first imaging modality used in the evaluation of suspected or diagnosed MPS; it generally includes anteroposterior and lateral radiographs of the spine and allows the detection of gross anomalies (e.g.,
os odontoideum,
kyphoscoliosis,
platyspondyly and anterior vertebral beaking).
Functional radiography consists of flexion-extension lateral views and allows the detection and quantification of intervertebral instability [19].
In addition,
radiographic follow-up examinations are useful in the evaluation and monitoring of specific clinical problems such as kyphoscoliosis.
CT
CT is more accurate than other imaging modalities (such as radiography and MR imaging) for demonstrating vertebral bony changes and,
particularly,
for characterization of the odontoid process and atlantoaxial articulation.
Therefore,
it is fundamental in order to obtain a detailed anatomical situation before surgical treatment (Fig. 1, Fig. 2).
Furthermore,
it may be preferred in patients with limited cooperation.
MR imaging
MR imaging allows direct visualization of spinal cord and nerve roots as well as of soft tissues,
ligaments and meninges [8,
12].
It is considered the most accurate imaging method for visualization of the space available for the spinal cord and for detection of spinal damage [1,
8,
12].
Therefore,
it represents the imaging of choice for evaluating of complications of MPS (e.g.,
spinal stenosis,
spinal compression and myelopathy) (Fig. 3, Fig. 5) and monitoring the pathologic progression of the disease after surgery (Fig. 6).
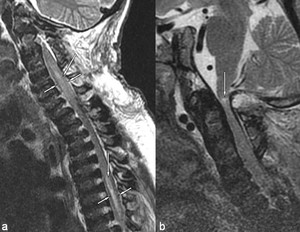
Fig. 6: Same patient as in Fig. 3. Sagittal MR images obtained seven days after suboccipital craniotomy and C1 laminectomy. a) T2-weighted image of cervicothoracic spine showing significant regression of spinal cord edema; focal areas of edema (arrows) associated with mild spinal cord thickening (small arrows) persist at C4-7 and mid-thoracic levels. b) T2-weighted image of cervical spine shows partial regression of the small area of intramedullary increased signal due to compressive myelopathy (arrow).
References: Leone A et al. (2015) Spinal Involvement in mucopolysaccharidoses: a review. Childs Nerv Syst 31:203-212.

, thoracolumbar kyphosis, and posterior vertebral scalloping (small arrows). Note retrolisthesis of the beak-shaped L3 vertebra. References: Leone A et al. (2015) Spinal Involvement in mucopolysaccharidoses: a review. Childs Nerv Syst 31:203-212.")
 Sagittal reformatted CT images of the lumbar spine (a) and thoracolumbar junction (b) show some typical thoracolumbar spine changes including platyspondyly, anterior beaking within the midportion of the vertebral bodies (small arrows in a and b) and posterior scalloping of the vertebral bodies (arrows in a and b). References: Leone A et al. (2015) Spinal Involvement in mucopolysaccharidoses: a review. Childs Nerv Syst 31:203-212.")
. Increased signal intensity within the cervical cord from C3 to C7, consistent with edema, is clearly evident as well as mild spinal cord thickening (small arrows). Note odontoid hypoplasia and localized thickening of the surrounding tissue (*). References: Leone A et al. (2015) Spinal Involvement in mucopolysaccharidoses: a review. Childs Nerv Syst 31:203-212.")
 Transverse T2-weighted MR image passing through T4 vertebra shows spinal cord edema with central gray matter involvement (circle). b) Transverse T1-weighted MR image passing through T8 vertebra shows thickness of the flaval ligament on the right encroaching on the dural sac (small arrows). References: Leone A et al. (2015) Spinal Involvement in mucopolysaccharidoses: a review. Childs Nerv Syst 31:203-212.")
. Increased signal intensity within the thoracolumbar cord, consistent with edema, is clearly evident as well as mild spinal cord thickening (small arrows). Note thoracolumbar kyphosis, platyspondyly, and sternum deformity. References: Leone A et al. (2015) Spinal Involvement in mucopolysaccharidoses: a review. Childs Nerv Syst 31:203-212.")
 T2-weighted image of cervicothoracic spine showing significant regression of spinal cord edema; focal areas of edema (arrows) associated with mild spinal cord thickening (small arrows) persist at C4-7 and mid-thoracic levels. b) T2-weighted image of cervical spine shows partial regression of the small area of intramedullary increased signal due to compressive myelopathy (arrow). References: Leone A et al. (2015) Spinal Involvement in mucopolysaccharidoses: a review. Childs Nerv Syst 31:203-212.")