SCAN PROTOCOL
- MRAs were scanned in the same session on 3T unit (Discovery MR750w 3.0T,
GE Healthcare,
Milwaukee,
WI,
U.S.A.).
- Silent MRA : TR/TE,
1116.4/0.016 msec; flip angle,
5°; field of view,
180×180 mm; matrix,
150×150; section thickness,
1.2 mm; number of excitations (NEX),
1.5; band width,
±20 kHz; and acquisition time,
7 min 40 s.
- TOF MRAs : TR/TE,
19/2.9 msec; flip angle,
15°; field of view,
200×200 mm; matrix,
416×192; section thickness,
1.2 mm; NEX,
1; band width,
±41.7 kHz; and acquisition time,
3 min 31 s.
- In some patients,
DSA was performed with the following angiographic systems: AXIOM Artis dTA (Siemens AG,
Erlangen,
Germany) until February 2014 and Artis Q BA Twin (Siemens AG).
CASEs
- Hereby,
comparing with TOF-MRA and DSAs,
clinical application of SILENT MRA in several vascular disease were presented
1) Brain aneurysms,
stent assisted coil embolization
Fig. 3: phantom model of stent-assisted coil embolization
References: Neuronews
- There is a limitation to evaluate a precise recanalization even with an angiogram
- Prevalence of late in-stent stenosis is 5% (0.8~20%)
- Need to establish a reliable method for restenosis of recanalization
Case 1) A case with Right ICA aneurysm treated with SACE on her 40's. Stent was deployed between the yellow arrows. Dephasing due to a susceptibility effect was reduced. Out pouching of stented part and in-stent flow was evident on Silent MRA.
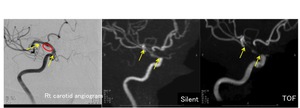
Fig. 4: DSA, SILENT MRA and TOF-MRA of post SACE patient for rt ICA aneurysm
Case 2) A case with Left ICA aneurysm treated with SACE on her 60's. Even with a carotid angiogram,
recanalized flow between the coil mass and stent is difficult to demonstrate. Though TOF showed signal loss at the region,
Silent showed the flow.
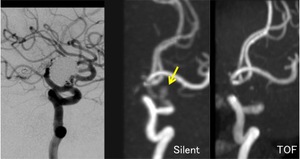
Fig. 5: DSA, SILENT MRA and TOF-MRA of post SACE patient for rt ICA aneurysm
Case 3) Y-stent graft deployment was performed for basilar tip aneurysm on her 60's.
A proportion of deployed stents were traced as red and yellow-line.
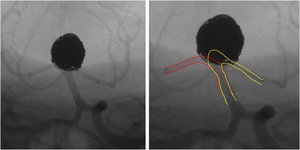
Fig. 6: DSA images during Y-graft deployment for BA-tip aneurysm
SILENT MRA showed an in-stent flow and residual flow inside the aneurysm.
On the other hand,
TOF-MRA could not depict neither in-stent flow,
nor residual flow.
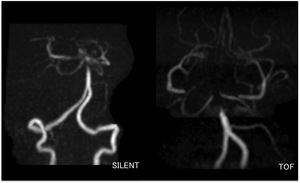
Fig. 7: SILENT MRA and TOF-MRA of post SACE patient for BA-tip aneurysm
2) Brain aneurysms,
PIPELINE deployment +/- coil
- PIPELINE stent deployment is widely used in these days.
- In patients with fragile aneurysmal wall,
additional coil embolization is taken into consideration.
Case 4) PIPELINE deployment with coil embolization for large ICA-opthalamic aneurysm on her 40's.
DSA obscured the filling of remnant flow in the aneurysmal sac,
however,
SILENT MRA could depict it.
Note that SILENT MRA could also represent a detailed kinking of opthalamic artery,
regardless of neighboring metellic materials.
On SILENT MRA,
in-PIPELINE flow depiction is more evident compared with TOF-MRA.
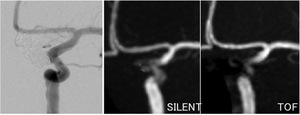
Fig. 8: DSA, SILENT MRA and TOF-MRA of post PIPELINE assisted coil embolization for lt ICA aneurysm
3) Subarachnoid hemorrhage
- SAH is mostly found on CT.
- In survey for ruptured aneurysm,
MRA is commonly used.
Especially in basal cistern,
we sometimes experience an unclear MRA,
because of T1-shortening effect of acute hematoma on TOF-MRA.
- By using a T1-weighted image subtraction technique,
SILENT provide a hematoma-removed MR angiography images.
Case 5) Acute subarachnoid hemorrhage during coil embolization for rt IC-PC aneurysm on his 60's.
Rapid coil embolization was performed and post operative MRI was scanned.
Complete occlusion of the aneurysm was confirmed on SILENT MRA.
TOF-MRA could not provide useful information regarding the remnancy or recurrent of aneurysm rupture.
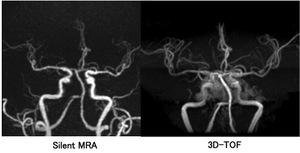
Fig. 9: SILENT MRA and TOF-MRA ofSAH patient
4) Thrombosed brain aneurysm
- Thrombosed aneurysm shows several signal intensity on conventional MR images.
- It sometimes misdiagnosed with large,
patent aneurysm or other neoplasm.
- SILENT MRA shows true flow,
and eliminates the possibility to misdiagnosis.
case 6) A female diagnosed left MCA aneurysm on her 60's.
She had been believed to have a flow inside the aneurysm,
and for the tratment,
transfered to our hospital.
No aneurysmal flow was detected on SILENT-MRA.
It indicates that there is in-sac flow.
No furrther treatment is needed.
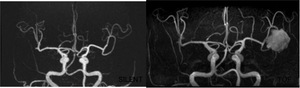
Fig. 10: SILENT MRA and TOF-MRA for lt MCA aneurysm
5) Moyamoya disease
- Moyamoya syndrome is a disease in which certain arteries in the brain are constricted.
Blood flow is blocked by the constriction,
and also by blood clots.
- A
 collateral circulation develops around the blocked vessels to compensate for the blockage,
but the collateral vessels are small,
weak,
and prone to hemorrhage, aneurysm and thrombosis.
On conventional X-ray angiography,
these collateral vessels have the appearance of a "puff of smoke".
collateral circulation develops around the blocked vessels to compensate for the blockage,
but the collateral vessels are small,
weak,
and prone to hemorrhage, aneurysm and thrombosis.
On conventional X-ray angiography,
these collateral vessels have the appearance of a "puff of smoke".
case 7) A female on her 10's.
On SILENT-MRA,
moyamoya vessel or collateral vessel are more evident compared with TOF-MRA.
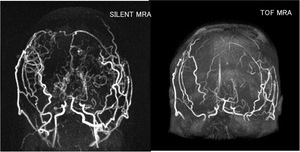
Fig. 11: SILENT MRA and TOF-MRA of moyamoya disease
6) Clipping and bypass
- Aneurysmal clipping combined with high-flow bypass is established operation method for large internal carotid aneurysm.
- Bypass patency is a key findings for a present or future ischemic stroke.
- % of patients have restenosis or collapse of bypass graft.
case 8) A female on her 60's with giant rt ICA aneurysm.
Rt ICA ligation with clip and STA-MCA bypass was performed previously.
She has no past history of ischemic attack after the surgery.
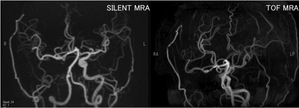
Fig. 12: SILENT MRA and TOF-MRA of patients treated with ICA ligation and bypass
On Silent MRA,
we could delineate a bypass route between a STA and a opercular branch of MCA.
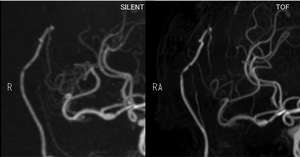
Fig. 13: Magnified view of SILENT and TOF MRAs
7) Cavenous sinus dural AVF
case 9) Female on her 40’s.
During left ICA anuersm embolization.
CCF was occurred during a prosedure.

Fig. 14: DSA images during lt ICA aneurysm coiling
Different from TOF,
Silent could demonstrate a caudal flow clearly (yellow arrow).
TOF-MRA has a strong point to depict a cranial direction of flow,
however,
sometimes have a signal loss of caudal direction flow.
This is a example to show a tolerance of SILENT-MRA in any flow-direction.
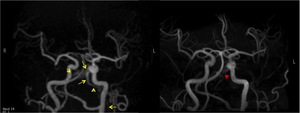
Fig. 15: SILENT MRA and TOF-MRA of lt CCF
8) Large AVM
- AVM is is an abnormal connection between arteries and veins,
bypassing the capillary system.
- This vascular anomaly is widely known because of its occurrence in the central nervous system,
but can appear in any location.
Although many AVMs are asymptomatic,
they can cause intense pain or bleeding or lead to other serious medical problems.
case 10) SILENT-MRA could demonstrate each vessel clearly,
especially deep part of AVM.
It might provide an useful information for preoperative planning for surgery.
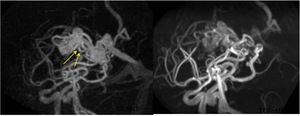
Fig. 16: SILENT and TOF-MRA for large AVM
9) Small AVM
case 11) Male on her 40’s.
An AVM located at lt.
occipital lobe was removed 3 years ago.
Because of its location (visual cortex),
total removal was avoided on purpose. To confirm the remnant AVM,
the patient came to the MR unit. Only SILENT could depict the small vascular structure that continues to a cotton-wool like high signal.
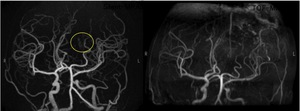
Fig. 17: SILENT MRA and TOF-MRA of remnant AVM of occipital lobe
Similar to the angiogram,
recurrent feeding artery and small nidus was demonstrated on SILENT MRA.
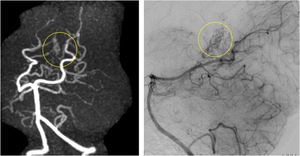
Fig. 18: magnified view of SILENT MRA and DSA image
