Spondylolysis is an osseous defect of the pars interarticularis,
thought to be a developmental or acquired stress fracture secondary to chronic low-grade trauma (Fig. 1).
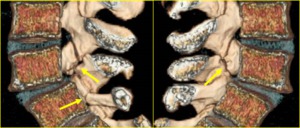
Fig. 1: 3D CT reconstructed images of chronic non-united pars fractures (arrows) in an 18-year-old elite soccer player.
References: Institute of Radiology, Catholic University, School of Medicine, Rome/Italy.
Pathogenesis
The mechanism of injury is usually a combination of repetitive flexion,
extension,
or rotation of the lumbar spine [1,
2].
In particular,
the pars interarticularis of L5 is sheared during extension by the inferior articular process of L4 and the superior articular process of the sacrum acting as a pair of wedges.
This mechanism leads to stretching of the pars and eventually to a stress microfracture.
With continued stress an overt but incomplete fracture occurs that may progress to complete fracture and chronic non-union osseous defect of the pars interarticularis.
Principles of biomechanics: Spino-pelvic balance
The human standing posture involves a delicate balance between the spine and pelvis.
A balanced posture is obtained when these body segments are aligned in order to minimize energy expenditure [3] (Fig. 2).
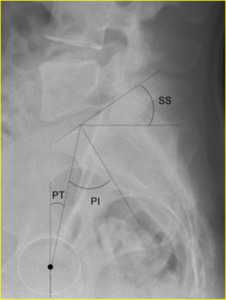
Fig. 2: Lateral radiograph of the lumbosacral spine shows the following spino-pelvic parameters: the pelvic incidence (PI), the pelvic tilt (PT), and the sacral slope (SS). PI is the angle formed by drawing a perpendicular line starting from the midpoint of the sacral end plate and a line connecting this point to the middle axis of the femoral heads. PT is the angle between the vertical line and the line connecting the midpoint of the sacral plate to the axis of the femoral heads. SS is the angle between the superior plate of S1 and the horizontal line.
References: Leone A et al. (2011) Lumbar spondylolysis: a review. Skeletal Radiol 40:683–700.
Development of spondylolisthesis
Spondylolysis diminishes the stabilizing ability of the posterior elements in the spinal motion segment and may lead to isthmic spondylolisthesis [4,5].
Thus,
there is strong support to assume that spondylolysis can induce spinal segmental instability/hypermobility in the growing adolescent spine.
The pathomechanism of slippage in pediatric spondylolysis has been hypothesized as follows: at first,
spondylolysis changes the spine kinematics leading to stress concentration at the growth plate during lumbar motion.
Over time,
the accumulation of the stresses may lead to physis stress fracture at the vertebral body and eventually spondylolisthesis [6].
The parameters of sagittal spino-pelvic balance are disturbed in adolescents and young adults with isthmic spondylolisthesis.
These subjects stand with an increased SS,
PT,
PI,
and lumbar lordosis,
but with a decreased thoracic kyphosis [7,8].
A high PI is a predisposing factor for L5 spondylolisthesis because high PI will necessarily predispose to a high SS and/or PT and to increased lumbar lordosis.
Thus,
increased lumbar lordosis associated with L5 spondylolisthesis should be secondary to the high PI and is an important factor causing high shear stresses at the L5 pars interarticularis [8].

 in an 18-year-old elite soccer player. References: Institute of Radiology, Catholic University, School of Medicine, Rome/Italy.")
, the pelvic tilt (PT), and the sacral slope (SS). PI is the angle formed by drawing a perpendicular line starting from the midpoint of the sacral end plate and a line connecting this point to the middle axis of the femoral heads. PT is the angle between the vertical line and the line connecting the midpoint of the sacral plate to the axis of the femoral heads. SS is the angle between the superior plate of S1 and the horizontal line. References: Leone A et al. (2011) Lumbar spondylolysis: a review. Skeletal Radiol 40:683–700.")