Mechanism of injury,
location and types of fractures in AS patients
Interestingly,
fractures in AS patients have the following distinctive characteristics:
- the majority of fractures occur after low-energy trauma [1,
2,
6,
12-14]: due to its changed biomechanical properties,
the forces needed to fracture an ankylosed spine are smaller than those required to fracture a normal spine.
Therefore,
in the AS spine even a trivial trauma (i.e.
falls from standing/sitting position) can result in a fracture of the vertebral body or its other components.
Sometimes,
fractures can occur without any recognizable trauma;
- hyperextension is the most frequently observed mechanism of injury [2,
12];
- the lower cervical spine is the most commonly injured area because of its increased mobility,
small vertebral bodies,
oblique articular facets and the mobility of the skull on it [2-4,
15];
- AS-related fractures usually pass through the vertebral body (transvertebral fractures) (Fig. 2) or through the intervertebral disk (transdiskal fractures) (Fig. 3) because of extensive osteopenic changes and loss of elasticity of the disks [2,
4,
12,
13,
15,
16];
- both the anterior and posterior elements of the vertebra are often involved (Fig. 3): as ossified ligaments and surrounding tissues are also damaged (Fig. 3c),
fractures of the ankylosed spine tend to be highly unstable and may be associated with neurological complications [1,
2,
4-6,
10-16].
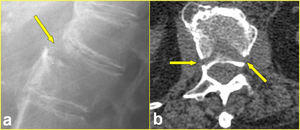
Fig. 2: Lumbar transverse fracture in a 65-year-old woman after a fall from sitting position. a) Lateral radiograph of the thoracolumbar spine shows the fracture through L1 vertebral body (arrow). b) Axial CT scan confirms the fracture extending to the middle column (arrows).
References: Institute of Radiology, Catholic University, School of Medicine, Rome/IT
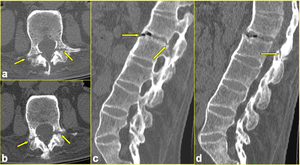
Fig. 3: The same patient as in Fig. 1. a, b) Axial CT scans passing through L2 vertebra reveal bilateral non-displaced fracture at L2 pedicle-articular pillar junction (arrows in a and b). c, d) Sagittal multiplanar reformatted CT images clearly define the transverse intradiskal fracture involving the anterior and posterior longitudinal ligaments (arrows in c) and extending to posterior elements (arrow in d).
References: Institute of Radiology, Catholic University, School of Medicine, Rome/IT
Imaging modalities and findings
Imaging of the spine plays a crucial role in the management of AS patients allowing an early detection of vertebral fractures and reducing the high rate of mortality and morbidity in such patients.
Radiography
Even when a fracture is clinically suspected,
diagnosis can be difficult on the basis of radiography alone,
given the highly abnormal spinal structure in patients with AS (ossified ligaments,
surrounding osseous proliferation,
poor outlining of the disk space,
osteoporosis) [1,
3,
5,
6,
10,
13,
17].
Furthermore,
the possibility to detect fractures located in the lower cervical spine or fractures of the thoracic neural arch and its pedicles is reduced due to projection of the shoulder girdle [1,
3,
4,
6,
10] (Fig. 4).
The use of CT and MR imaging has been shown to increase the sensitivity of initial radiographic assessment [2,
6,
10,
12,
13].
Accordingly,
CT should be used to image the spine whenever a patient with AS presents with new onset neck or back pain,
no matter how minor or trivial the reported trauma,
as it can demonstrate vertebral fractures in detail [1,
6,
12] (Fig. 4a).
Sometimes the suspicion of a fracture on radiography raises when the bony bridging due to the ossification of the anterior and posterior longitudinal ligament is incomplete (Fig. 1).
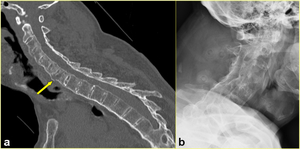
Fig. 4: 49-year-old-man with AS after a fall from a scaffold. a) Sagittal multiplanar reformatted CT image shows transverse fracture through the C7 vertebral body involving the ossified anterior and posterior longitudinal ligaments (arrow). b) Lateral radiograph does not show the lesion.
References: Institute of Radiology, Catholic University, School of Medicine, Rome/IT
CT
CT of the spine is considered the reference standard for showing bony details,
including fractures and fragments in patients with spinal fractures and AS.
The new generation CT scanners with multiplanar reconstructions and three-dimensional (3D) volume rendered images can provide information regarding the extent of the lesion and help in visualization of the details of these fractures [12] (Fig. 2, Fig. 3, Fig. 4a, Fig. 5, Fig. 6,
and Fig. 7).
The most relevant sign of AS fractures is widening of the intervertebral space.
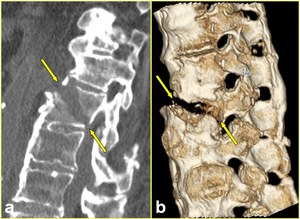
Fig. 5: The same patient as in Fig. 2. a) Sagittal reformatted, and b) 3D volume-rendered CT images better define the through-and-through fracture involving the ossified anterior longitudinal ligament and the body of L1 to its posterior cortex (arrows in a, and b). Note the ankylosis of posterior spinal elements in b.
References: Institute of Radiology, Catholic University, School of Medicine, Rome/IT
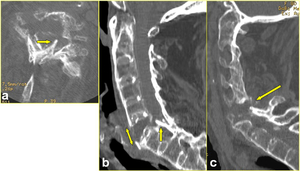
Fig. 6: Transverse fracture of C6 vertebra in a 70-year-old woman, after a fall from standing height, complicated by paralysis in both arms and paresis in both legs. a) Axial CT scan passing through C6 vertebra, b) midsagittal, and c) sagittal to the right of the midline multiplanar reformatted CT images show the highly displaced nature of the fracture involving all three columns of C6 vertebra. Note the severe vertebral osteoporosis, the laminar fragment encroaching the spinal cord (arrow in a, and b), the disruption of ossified anterior longitudinal ligament (double-head arrow in b), and the flaval ligament tear (arrow in c).
References: Institute of Radiology, Catholic University, School of Medicine, Rome/IT
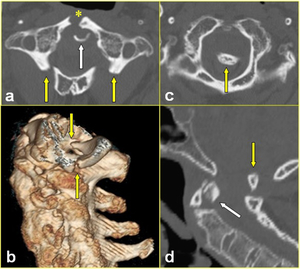
Fig. 7: High dens fracture associated with a Jefferson bursting fracture in a 63-year-old man with AS after a fall down. a) Axial CT scan shows the high dens fracture (white arrow) and the Jefferson bursting fracture with only a single fracture of the anterior arch (*), and bilateral fracture of the posterior arch (yellow arrows). b) Sagittal 3D volume-rendered CT image shows the cranial displacement of the posterior arch fragment (arrows). c) Axial CT scan passing through the foramen magnum and d) sagittal multiplanar reformatted CT image demonstrate the displacement of the posterior arch fragment into the foramen magnum causing brainstem encroachment (yellow arrow in c, and d). The high dens fracture is well evident in d (white arrow). This injury was complicated by tetraplegia.
References: Institute of Radiology, Catholic University, School of Medicine, Rome/IT
Magnetic resonance (MR) Imaging
Many reports in the literature suggest the presence of neurological complications after vertebral fractures in patients with AS,
including spinal cord and nerve root lesions,
intramedullary edema,
and paravertebral hematomas resulting in a variable degree of sensory and/or motor deficits [2,
6,
12,
18] (Fig. 6,
Fig. 7,
Fig. 8, Fig. 9,
and Fig. 10).
Alaranta et al.
[18] determined that the incidence of spinal cord injuries (SCI) in patients with AS was 11.4 times that in the population at large.
The higher incidence of SCI in AS is,
of course,
correlated with the increased incidence of spinal fractures in these patients,
but also directly related to the AS disease process.
In fact,
ossified spinal ligaments also fracture as part of the injury pattern,
further decreasing the structural support available to the spine [1].
MR imaging is an excellent tool to evaluate soft tissues such as spinal ligaments,
joint capsules and nervous structures,
so it is considered the modality of choice to detect neurologic complications and a reasonable option to exclude occult fractures undetected by multi-detector CT [3,
13,
10,
17] (Fig. 8,
Fig. 9b-c,
and Fig. 10).
Bone and soft tissue near the fracture line become edematous for some time after trauma and increased signal intensity is readily detected on fluid sensitive fat-suppressed sequences,
i.e.
short-tau inversion recovery (STIR) or fat-saturated T2-weighted images (Fig. 8c).
The fracture line appears as a linear area of low signal intensity on both T1 and T2 sequences,
unless fluid collection or hematoma are present inside the fracture line [12] (Fig. 10).
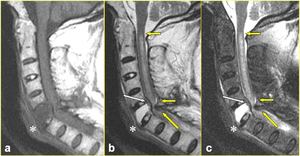
Fig. 8: The same patient as in Fig. 6. a) Sagittal T1-weighted, b) corresponding T2-weighted, and c) fat-suppressed T2-weighted images confirm the acute fracture of C6 vertebra with extensive vertebral body edema and retropulsion, and define the position of the laminar fragment relative to the spinal cord (yellow arrow in b, and c). The resultant cord contusion that spans five vertebral levels is seen on the T2-weighted images (small arrow in b, and c). Posterior longitudinal ligament stretching (white arrow in b, and c), and a heterogeneous prevertebral hematoma (* in a, b, and c) resulting from the anterior longitudinal ligament disruption are also evident.
References: Institute of Radiology, Catholic University, School of Medicine, Rome/IT

Fig. 9: The same patient as in Fig. 7. a) Sagittal multiplanar reformatted CT image shows, in addition to the already-mentioned fractures, chronic C5 and C6 fracture with ankylosis of the vertebral bodies forming a single vertebral block (arrow), and mild retropulsion of posterior wall fragment. Increase in the C4-5 interlaminar and interspinous distance reflects a posterior ligament complex tear (double-head arrow). b) Sagittal T2-weigthed MR image confirms the brainstem encroachment (yellow arrow) as well as the C5-6 vertebral body collapse (white arrow), with no evidence of signal changes in the cord. Due to the respiratory compromise, the patient had difficulty in remaining immobile during the examination. c) Sagittal T2-weighted MR image of the thoracolumbar spine showing chronic compression fracture of T12 vertebral body (*). Note the marrow signal is normal. The patient remained a complete tetraplegic until his death 9 days later for respiratory insufficiency.
References: Institute of Radiology, Catholic University, School of Medicine, Rome/IT
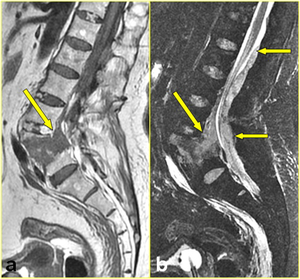
Fig. 10: Transverse comminuted fracture of L5 vertebra with severe anterior displacement of the spine in a 56-year-old man after a simple fall. The patient was neurologically intact, with the sole complaint of lower back pain. a) Sagittal T1-weighted and b) corresponding fat-suppressed T2-weighted images show the fracture gap and the anterior subarachnoid space presenting with a low signal on T1-weighted image and a high signal on T2-weighted image (arrow in a, and b) (the signal of hematomas within the fracture gaps may vary with age). Note a heterogeneous dorsally located epidural collection extending from L1 to L5, which represents a spinal epidural hematoma (small arrows in b).
References: Institute of Radiology, Catholic University, School of Medicine, Rome/IT

 Lateral radiograph of the thoracolumbar spine shows the fracture through L1 vertebral body (arrow). b) Axial CT scan confirms the fracture extending to the middle column (arrows). References: Institute of Radiology, Catholic University, School of Medicine, Rome/IT")
 Axial CT scans passing through L2 vertebra reveal bilateral non-displaced fracture at L2 pedicle-articular pillar junction (arrows in a and b). c, d) Sagittal multiplanar reformatted CT images clearly define the transverse intradiskal fracture involving the anterior and posterior longitudinal ligaments (arrows in c) and extending to posterior elements (arrow in d). References: Institute of Radiology, Catholic University, School of Medicine, Rome/IT")
 Sagittal multiplanar reformatted CT image shows transverse fracture through the C7 vertebral body involving the ossified anterior and posterior longitudinal ligaments (arrow). b) Lateral radiograph does not show the lesion. References: Institute of Radiology, Catholic University, School of Medicine, Rome/IT")
 where the bony bridging is incomplete. This sign raised the suspicion of a fracture (Fig. 3). References: Institute of Radiology, Catholic University, School of Medicine, Rome/IT")
 Sagittal reformatted, and b) 3D volume-rendered CT images better define the through-and-through fracture involving the ossified anterior longitudinal ligament and the body of L1 to its posterior cortex (arrows in a, and b). Note the ankylosis of posterior spinal elements in b. References: Institute of Radiology, Catholic University, School of Medicine, Rome/IT")
 Axial CT scan passing through C6 vertebra, b) midsagittal, and c) sagittal to the right of the midline multiplanar reformatted CT images show the highly displaced nature of the fracture involving all three columns of C6 vertebra. Note the severe vertebral osteoporosis, the laminar fragment encroaching the spinal cord (arrow in a, and b), the disruption of ossified anterior longitudinal ligament (double-head arrow in b), and the flaval ligament tear (arrow in c). References: Institute of Radiology, Catholic University, School of Medicine, Rome/IT")
 Axial CT scan shows the high dens fracture (white arrow) and the Jefferson bursting fracture with only a single fracture of the anterior arch (*), and bilateral fracture of the posterior arch (yellow arrows). b) Sagittal 3D volume-rendered CT image shows the cranial displacement of the posterior arch fragment (arrows). c) Axial CT scan passing through the foramen magnum and d) sagittal multiplanar reformatted CT image demonstrate the displacement of the posterior arch fragment into the foramen magnum causing brainstem encroachment (yellow arrow in c, and d). The high dens fracture is well evident in d (white arrow). This injury was complicated by tetraplegia. References: Institute of Radiology, Catholic University, School of Medicine, Rome/IT")
 Sagittal T1-weighted, b) corresponding T2-weighted, and c) fat-suppressed T2-weighted images confirm the acute fracture of C6 vertebra with extensive vertebral body edema and retropulsion, and define the position of the laminar fragment relative to the spinal cord (yellow arrow in b, and c). The resultant cord contusion that spans five vertebral levels is seen on the T2-weighted images (small arrow in b, and c). Posterior longitudinal ligament stretching (white arrow in b, and c), and a heterogeneous prevertebral hematoma (* in a, b, and c) resulting from the anterior longitudinal ligament disruption are also evident. References: Institute of Radiology, Catholic University, School of Medicine, Rome/IT")
 Sagittal multiplanar reformatted CT image shows, in addition to the already-mentioned fractures, chronic C5 and C6 fracture with ankylosis of the vertebral bodies forming a single vertebral block (arrow), and mild retropulsion of posterior wall fragment. Increase in the C4-5 interlaminar and interspinous distance reflects a posterior ligament complex tear (double-head arrow). b) Sagittal T2-weigthed MR image confirms the brainstem encroachment (yellow arrow) as well as the C5-6 vertebral body collapse (white arrow), with no evidence of signal changes in the cord. Due to the respiratory compromise, the patient had difficulty in remaining immobile during the examination. c) Sagittal T2-weighted MR image of the thoracolumbar spine showing chronic compression fracture of T12 vertebral body (*). Note the marrow signal is normal. The patient remained a complete tetraplegic until his death 9 days later for respiratory insufficiency. References: Institute of Radiology, Catholic University, School of Medicine, Rome/IT")
 Sagittal T1-weighted and b) corresponding fat-suppressed T2-weighted images show the fracture gap and the anterior subarachnoid space presenting with a low signal on T1-weighted image and a high signal on T2-weighted image (arrow in a, and b) (the signal of hematomas within the fracture gaps may vary with age). Note a heterogeneous dorsally located epidural collection extending from L1 to L5, which represents a spinal epidural hematoma (small arrows in b). References: Institute of Radiology, Catholic University, School of Medicine, Rome/IT")