Imaging methods
If patients with gallbladder carcinoma present with abdominal distension or right upper quadrant pain,
abdominal plain film may be the first examination.
Gallstones or a porcelain bladder may be observed or in some cases,
calcified precipitated mucus within the neoplastic tissue.
If the tumor invades the adjacent bowel and fistulas are formed,
abnormal gas collections may be seen in the right upper quadrant or in the biliary tree.
[1,
7]
Sonography represents the first imaging technique used when a gallbladder disease is suspected,
due to its high availability,
but it is limited for an early diagnosis or for accurate staging.
[3,
7]
Computed tomography and magnetic resonance imaging are nowadays widely used for an exact characterization of potentially malignant gallbladder conditions,
for their staging and for their preoperative aspects.
The CT scan technique includes a preliminary nonenhanced evaluation of the abdomen,
followed by an evaluation of the abdomen during intravenous injection of non-ionic,
iodinated contrast medium in an arterial and portal venous phase. Sagittal and coronal multiplanar reconstructions are essential for distinguishing between tumors and benign wall thickening,
especially when they are located inferiorly,
but also in determining the relationship between the gallbladder cancer and the surrounding organs.
[2,
5]
MRI protocols include T2-weighted sequences (usually fast spin-echo sequences with respiratory gating),
which are optimal for assessing soft tissue abnormalities involving the gallbladder wall.
Heavily T2-weighted fluid sensitive acquisition techniques,
such as half-fourier acquisition single-shot turbo spin echo (HASTE), may be also used.
A better characterisation of the gallbladder,
bile ducts and adjacent liver parenchyma may be obtained with dynamic contrast enhanced fat-supressed T1-weighted MRI sequences.
In addition,
DWI (diffusion weighted imaging) with tri-directional diffusion gradients using three b values,
applied within a single acquisiton,
is routinely performed.
DWI has been studied for its capability in differentiating malignant from benign lesions in various abdominal organs,
including the gallbladder.
Due to its high cellularity,
gallbladder carcinoma will exhibit significant diffusion restriction,
with high signal on high b value DWI and low ADC signal.
[5]
Imaging patterns
Mass replacing the gallbladder
In 40-65%of cases,
gallbladder carcinoma presents as a mass replacing the gallbladder and often invading the adjacent liver parenchyma.
At ultrasonography,
the echotexture of this pattern is heterogeneous and reflects varying degrees of tumor necrosis.
Echogenic foci may also occur,
due to gallstones,
mural or tumoral calcifications but also anechoic foci of trapped bile or necrotic tissue.
Direct extension to the liver and biliary tree may also be visualized,
making the tumor inseparable from the adjacent hepatic parenchyma.
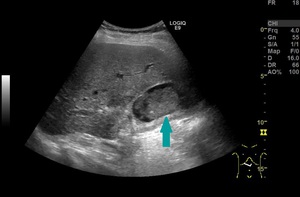
Fig. 1: Ultrasound of the abdomen - mass ocuppying the gallbladder (blue arrow)
References: Prof. Dr. Radu. Badea, Cluj - Napoca
On unenhanced CT,
gallbladder carcinoma appears as a hypodense or isodense mass,
occupying the gallbladder fossa and usually invading the adjacent liver parenchyma,
mostly the medial segment of the left lobe.
The tumor may contain nodular,
hypodense areas of necrosis and 40% of the lesions may show hypervascular foci of peripheral enhancement.
Calcifications in the gallbladder or in the tumor can be clearly defined with CT and associated findings include biliary obstruction and lymph node metastasis.
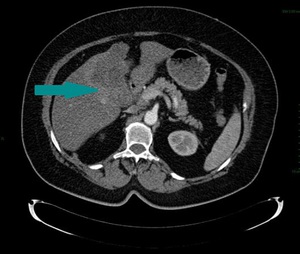
Fig. 2: Abdominal CT, axial image, contrast enhanced, arterial phase - large mass replacing the gallbladder (blue arrow)
References: Dr. Cosmin Caraiani, Cluj - Napoca
On MRI,
gallbladder carcinoma is usually hypo- to isointense on T1-weighted and shows moderately hyperintense signal characteristics on T2-weighted sequences.
On contrast enhanced images,
tumors will enhance mainly peripherally on the arterial phase,
but also fibrous stromal components can retain contrast during portal and delayed phases.
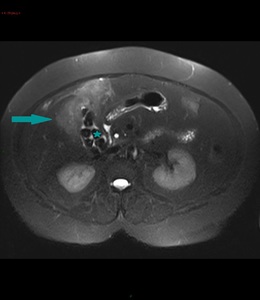
Fig. 3: MRI of the abdomen, axial image, HASTE sequence - mass partially ocuppying the gallbladder (blue arrow); gallstones (blue star); gallbladder wall not distinguishable
References: Dr. Cosmin Caraiani, Cluj - Napoca
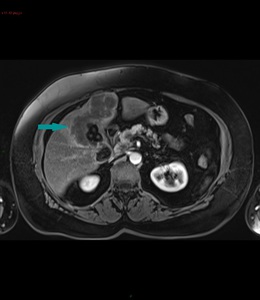
Fig. 4: Abdominal MRI, axial image, contrast enhanced sequence, portal venous phase - large mass with peripheral enhancement, replacing the gallbladder (blue arrow); gallstones
References: Dr. Cosmin Caraiani, Cluj - Napoca
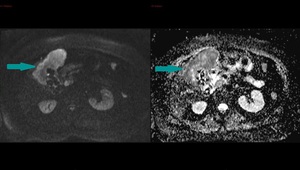
Fig. 5: Abdominal MRI, axial images, DWI sequence in a high b value (800) on the left and ADC map on the right - large mass replacing the gallbladder with a high signal on DWI (blue arrow on the left) and low signal on the ADC map (blue arrow on the right), showing a pattern of restricted diffusion
References: Dr. Cosmin Caraiani, Cluj - Napoca
Without being specific in distinguishing primary tumors from other malignant lesions,
an intense accumulation of 18F-FDG in the region of the gallbladder at PET is highly suggestive for malignancy.
[1,
2,
3]
Wall thickening
In 20-30% of cases,
gallbladder cancer may present as a focal or diffuse wall thickening.
This pattern is the most challenging,
because it mimics the appearance of acute and chronic cholecystitis,
xanthogranulomatous cholecystitis and adenomyomatosis,
as well as diffuse hepatic or systemic diseases such as acute hepatitis,
portal hypertension,
and congestive heart failure.
Areas of wall thickening may be viewed sonographically,
but this pattern is not easy to detect.
Markedly thickened wall,
seen on US or nonenhanced CT,
associated with mural irregularity or marked asymmetry could raise concerns for malignancy or complicated cholecystitis.
Contrast-enhanced CT and MRI is extremely helpful for distinguishing between a tumoral and inflammatory condition.
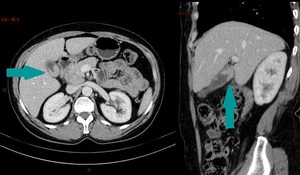
Fig. 6: CT of the abdomen, axial image on the left and sagittal reconstruction on the right, contrast enhanced images, portal venous phase - focal wall thickening of the gallbladder (blue arrow)
References: Dr. Cosmin Caraiani, Cluj - Napoca
Diffuse symmetric wall thickening favors a nonneoplastic process,
whereas asymmetric,
irregular or extensive thickening with marked enhancement during the arterial phase that persists or becomes isodense or isointense to the liver during the portal venous phase raises suspicion of gallbladder carcinoma.
Gallbladder cancer may also arise in a preexisting background of chronic cholecystitis,
which can make the diagnosis difficult or even delay it.
The association with lymphadenopathy,
extension into the liver or the presence of metastasis also suggets the diagnosis of gallbladder carcinoma.
MRI can be useful in cases of focal or diffuse mural thickening; it can distinguish carcinoma from chronic cholecystitis or adenomyomatosis.
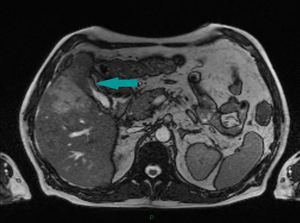
Fig. 7: Abdominal MRI, axial image, HASTE sequence - wall thickening of the gallbladder (blue arrow) extending into the adjacent liver parenchyma
References: Dr. Cosmin Caraiani, Cluj - Napoca
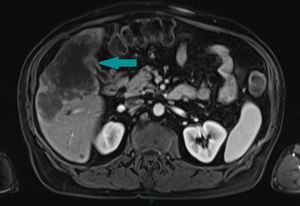
Fig. 8: MRI of the abdomen, axial image, contrast enhanced sequence, portal venous phase - gallbladder wall thickening with moderate enhancement (blue arrow) and extension into the adjacent liver parenchyma
References: Dr. Cosmin Caraiani, Cluj - Napoca
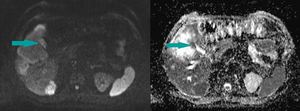
Fig. 9: Abdominal MRI, axial images, DWI sequence in high b value (800) on the left and ADC map on the right - gallbladder wall thickening showing a high signal on DWI (blue arrow on the left) and a low signal on ADC (blue arrow on the right) and extension into the adjacent liver parenchyma
References: Dr. Cosmin Caraiani, Cluj - Napoca
The contribution of FDG PET is limited in this setting because benign inflammatory lesions can accumulate FDG and result in false positive interpretations.
[1,
2,
3]
Intraluminal polyp
In 15-25% of cases,
gallbladder carcinoma can occur as a polypoid lesion,
which can be well-defined,
round or of oval shape.
Malignant polypoid lesions are usually larger than 1cm and may have thickened implantation base.
On sonography,
the malignant intraluminal mass is immobile with changes in patient position,
so it can be easily distinguished from sludge.
On CT scans,
malignant lesions may be hypodense or isodense and also subtle extension of the tumor beyond the wall of the gallbladder can be demonstrated.
On MR images,
the tumor demonstrates prolongation of the T1 and T2 relaxation times and ill-defined early enhancement at dynamic gadolinium-enhanced MRI represent its typical appearance.
[1,
2,
3]
Evaluation of tumor extension
Imaging methods
Sonography is helpful for detecting the primary tumor and adjacent liver invasion,
but it is not able to accurately depict the full extent of the disease.
Also,
potentially curable stage 1 cancers are difficult to identify with US.
Endoscopic US may accurately evaluate the depth of gallbladder cancer invasion.
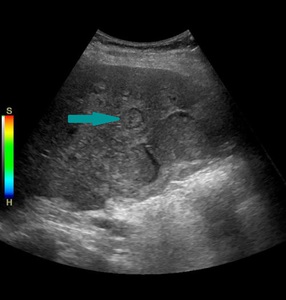
Fig. 10: Abdominal ultrasound showing multiple round, isoechoic lesions with hypoechoic rim (example marked with blue arrow) - liver metastasis in a patient with known gallbladder cancer
References: Prof. Dr. Radu. Badea, Cluj - Napoca
CT is more helpful for detecting lymph node involvement,
adjacent organ invasion and distant metastasis.
This imaging method is now widely available and has a reported accuracy up to 84% in determining the T stage of the primary tumor,
as well as 85% in demonstrating hepatic and vascular invasion,
lymphadenopathy and distant metastasis and thus,
predicting resectablity.
Unenhanced and iodinated contrast-enhanced studies during arterial and portal venous phases are obtained,
then multiplanar reconstructions may be generated,
providing an accurate vascular and presurgical view.
Direct,
percutaneous transhepatic or intraoperative cholangiography may be performed in uncertain cases or when therapeutic management is necessary.
Cholangiography may demonstrate malignant strictures involving the biliary tree and even depict intraluminal gallbladder filling defects or a mass displacing and invading the gallbladder.
MRI,
associated with cholangiographic and vascular phases may be up to 100% sensitive for detecting bile duct and vascular invasion.
Yet,
sensitivity for detecting hepatic invasion is only 67% and for lymph node metastasis only 56%.
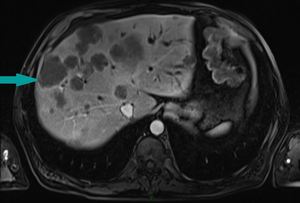
Fig. 11: MRI of the abdomen, axial image, contrast enhanced sequence, portal venous phase - liver metastasis (example marked with blue arrow), associated with bile duct dilatation, in a patient with known gallbladder cancer
References: Dr. Cosmin Caraiani, Cluj - Napoca
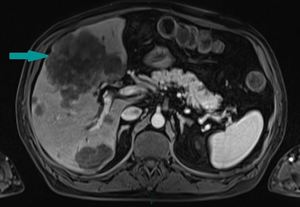
Fig. 12: Abdominal MRI, axial image, contrast enhanced sequence, portal venous phase - large liver metastasis (blue arrow) in a patient with known gallbladder cancer
References: Dr. Cosmin Caraiani, Cluj - Napoca
PET/CT may also have a promising role in the detection of unsuspected metastasis,
which may alter staging and therapy.
[1,
2,
3,
5,
7]
Extension patterns
The most common type of extension is direct extension to adjacent organs,
because of the thin gallbladder wall,
which lacks a lamina propria and has only one muscular layer.
Other possible extension paths are lymphatic,
vascular,
intraperitoneal,
intraductal and neural spread.
Direct extension involves the liver most frequently,
followed by the colon,
duodenum and pancreas.
Adjacent bowel invasion may be demonstrated with radiographic studies,
such as barium enema studies and upper gastrointestinal series.
CT and MRI can accurately depict the extension of the primary tumor into the liver or hepatoduodenal ligament.
CT findings of tumor invasion into the hepatoduodenal ligament include various nodular masses,
due to lymph nodes or adenopathy along the hepatoduodenal ligament or infiltrating soft tissue areas obscuring the portal vein.
Tumor extension has the same signal intensity as the primary tumor on MRI.
Another common finding in gallbladder carcinoma is biliary dilatation,
which occurs because of the tumor spread along the cystic duct to the extrahepatic bile duct,
lymph node enlargement or intraductal spread ot the tumor.
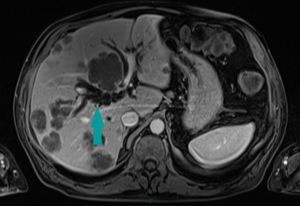
Fig. 13: MRI of the abdomen, axial image, contrast enhanced sequence, portal venous phase - bile duct dilation (blue arrow) due to tumoral compression in a patient with known gallbladder cancer and liver metastasis
References: Dr. Cosmin Caraiani, Cluj - Napoca
Lymphatic metastasis are common in gallbladder carcinoma.
They progress from the gallbladder fossa through the hepatoduodenal ligament to the nodal peripancreatic stations.
Malignant lymph nodes are usually greater than 10mm in short axis and have a peripheral or heterogeneous contrast material enhancement. Even if not all the regional lymph nodes are depicted with CT,
abnormally sized lymph nodes (>10mm) clearly suggest that lymphatic spread has occured.
Hematogeneous metastasis are most frequently seen in the liver.
More rarely,
pulmonary,
skeletal,
pancreatic,
renal,
adrenal,
cardiac and cerebral metastasis can occur.
Liver metastasis are accurately depicted by CT and MR imaging.
[1,
3]
Staging
Two classification systems are used for staging the gallbladder carcinoma,
TNM and modified Nevin.
T1 gallbladder carcinoma is confined to the lamina propria (T1A) or the muscular layer of the gallbladder (T1B),
T2 represents a tumor extending to the serosa,
T3 perforating the serosa or directly invading the liver or one of the adjacent organs (stomach,
duodenum,
colon,
pancreas,
omentum,
extrahepatic bile ducts) or T4 invading the portal vein,
the hepatic artery or multiple extrahepatic organs.
In more than 50% of the cases,
lymphatic spread is present at initial diagnosis.
N1 nodes are represented by the cystic,
pericholedochal,
hilar,
periduodenal,
peripancreatic and superior mesenteric nodes.
Portocaval,
interaortocaval and more distant nodes are considered M1 disease.
T1 lesions without nodal involvement are classified as stage IA,
while T2 lesions without nodal metastasis are classified as stage IB disease.
T3 lesions without nodal spread are stage IIA.
T1,
T2 or T3 lesions with nodal involvement N1 are staged IIB.
T4 lesions without distant metastasis are considered stage III.
Stage IV is represented by any lesion with distant metastasis.
[1,
3]
Differential diagnosis
For gallbladder tumors manifesting as diffuse gallbladder mural thickening,
the differential diagnosis includes common inflammatory and noninflammatory causes of wall thickening.
Noninflammatory causes are heart failure,
cirrhosis,
hepatitis,
hypoalbuminemia,
renal failure,
while inflammatory conditions are represented by cholecystitis.
Pericholecystic abscesses,
gallbladder necrosis or fistula formation may occasionally complicate acute cholecystitis,
simulating aggressive neoplastic processes.
When a focal mass,
lymphadenopathy,
hepatic metastasis and biliary obstruction are present,
gallbladder carcinoma should be suspected.
The features of xantogranulomatous cholecystitis,
a pseudotumoral inflammatory condition and gallbladder carcinoma may overlap,
making the differential diagnosis dificult.
Both conditions may present mural thickening,
infiltration of the surrounding fat,
hepatic involvement and lymphadenopathy.
Adenomyomatosis represents a tumorlike lesion of the gallbladder with no malignant potential,
which may involve the gallbladder in a focal or diffuse manner.
It consists of proliferated epithelial and mural elements and Rokitansky-Aschoff sinuses,
seen as proeminent foldings of the epithelium.
Adenomyomatosis can be seen at US as a focal or diffuse gallbladder mural thickening and echogenic or anechoic foci in the wall,
which may produce a ring-down reverberation artifact.
MR imaging can be useful for distinguishing between adenomyomatosis and gallbladder cancer,
due to its ability to visualize the Rokitansky-Aschoff sinuses.
The differential diagnosis for intraluminal polypoid tumors includes adenomatous,
hyperplastic and cholesterol polyps,
but also carcinoid tumors,
metastatic melanoma and hematoma within the gallbladder.
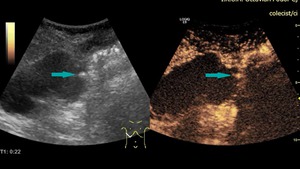
Fig. 14: Ultrasound and CEUS of the abdomen - benign gallbladder polyp (blue arrows), demonstrating contrast enhancement
References: Prof. Dr. Radu. Badea, Cluj - Napoca
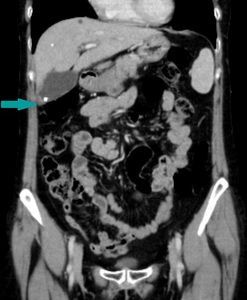
Fig. 15: CT of the abdomen, coronal reconstruction, contrast enhanced image, portal venous phase - benign gallbladder polyp (blue arrow), associated with gallstones
References: Dr. Cosmin Caraiani, Cluj - Napoca
When the tumor manifests as a mass replacing the gallbladder,
the differential diagnosis includes hepatocellular carcinoma,
cholangiocarcinoma and metastasis of the gallbladder.
Also,
lymph node masses around the distal bile duct and pancreatic head may mimic a pancreatic head carcinoma.
[1,
4]

 References: Prof. Dr. Radu. Badea, Cluj - Napoca")
 References: Dr. Cosmin Caraiani, Cluj - Napoca")
; gallstones (blue star); gallbladder wall not distinguishable References: Dr. Cosmin Caraiani, Cluj - Napoca")
; gallstones References: Dr. Cosmin Caraiani, Cluj - Napoca")
 on the left and ADC map on the right - large mass replacing the gallbladder with a high signal on DWI (blue arrow on the left) and low signal on the ADC map (blue arrow on the right), showing a pattern of restricted diffusion References: Dr. Cosmin Caraiani, Cluj - Napoca")
 References: Dr. Cosmin Caraiani, Cluj - Napoca")
 extending into the adjacent liver parenchyma References: Dr. Cosmin Caraiani, Cluj - Napoca")
 and extension into the adjacent liver parenchyma References: Dr. Cosmin Caraiani, Cluj - Napoca")
 on the left and ADC map on the right - gallbladder wall thickening showing a high signal on DWI (blue arrow on the left) and a low signal on ADC (blue arrow on the right) and extension into the adjacent liver parenchyma References: Dr. Cosmin Caraiani, Cluj - Napoca")
 - liver metastasis in a patient with known gallbladder cancer References: Prof. Dr. Radu. Badea, Cluj - Napoca")
, associated with bile duct dilatation, in a patient with known gallbladder cancer References: Dr. Cosmin Caraiani, Cluj - Napoca")
 in a patient with known gallbladder cancer References: Dr. Cosmin Caraiani, Cluj - Napoca")
 due to tumoral compression in a patient with known gallbladder cancer and liver metastasis References: Dr. Cosmin Caraiani, Cluj - Napoca")
, demonstrating contrast enhancement References: Prof. Dr. Radu. Badea, Cluj - Napoca")
, associated with gallstones References: Dr. Cosmin Caraiani, Cluj - Napoca")