SCAPULAR FRACTURES
Scapular fractures are rare and most often occur in the setting of high-energy chest trauma.
In clinical practice,
fractures of the scapula are generally divided into:
- Extraarticular fractures of the scapular body,
acromion,
or coracoid process,
that are treated nonsurgically.
- Fractures of the glenoid neck or articular surface,
that require surgical repair.
Fractures interesting the coracoid,
the scapular neck or body associated with fractures of the clavicle determine the clinical picture called "floating shoulder",
a complete instability of the shoulder girdle that requires surgical treatment.
INTRAARTICULAR FRACTURES OF THE GLENOID FOSSA may require surgical fixation (Fig.4).
Orthopedic surgeons use the system described by Ideberg for morphologic classification of these injuries [1].
- Type I fractures are vertically oriented fractures of the anterior or posterior glenoid rim.
- Type II–IV fractures are characterized by a transverse intraarticular fracture that exits through the lateral,
superior,
and medial scapular border,
respectively.
- Type V fractures are combinations of types II–IV.
- Type VI fractures are highly comminuted at the articular surface.
- Type VI fractures are often not reconstructible and are treated nonsurgically to preserve the remaining soft-tissue supports.
For type I–V fractures,
surgical fixation is suggested for intraarticular fractures with instability.
The Ideberg classification system for scapula fractures involving the glenoid fossa helps determine the need for surgical fixation of glenoid fossa fractures.
EXTRAARTICULAR FRACTURE OF THE GLENOID NECK involves either [2]:
- Glenoid anatomic neck fractures : almost always unstable,
and affected patients are therefore more likely to undergo surgery.
- Fractures of the glenoid surgical neck : managed differently depending on displacement. Fractures displaced less than 1 cm and angled less than 40° are managed nonsurgically.
Fractures displaced 1 cm or more or angled at least 40° in the coronal or transverse plane require surgical fixation.
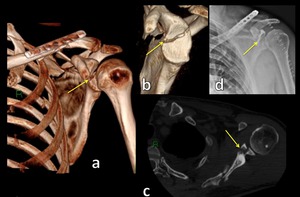
Fig. 4: 3D CT images (a,b) and axial CT scan (c) show intraarticular fracture of the glenoid fossa treated with surgical fixation (d).
References: Institute of Radiology, Catholic University - Rome/IT
GLENOHUMERAL DISLOCATION
The vast majority of traumatic glenohumeral dislocations are anterior,
and the remainder are usually posterior and inferior; superior dislocations are exceedingly rare.
ANTERIOR GLENOHUMERAL DISLOCATION
Anterior dislocation is common,
accounting for 85-98% of all dislocations (Fig.5,6) [3].
Anterior dislocations are subclassified according to the resting position of the humeral head relative to the glenoid into:
- subcoracoid (most common)
- subglenoid
- subclavicular
- intracoracoid
- supracoracoid
Anterior dislocations most commonly are due to indirect mechanisms,
as sudden loading of the arm in varying degrees of abduction,
external rotation,
and extension.
They are less commonly due to direct injury mechanisms after a impact to the posterior aspect of the shoulder .
Acute traumatic anterior dislocations are most commonly diagnosed clinically,
with initial imaging to confirm the clinical suspicion and characterize the type and resting position of the dislocation.
Multiple fractures and soft-tissue injuries are associated with anterior dislocations,
among the most commonly reported are injuries to the anteroinferior glenoid labrum and bony glenoid rim,
referred to as soft-tissue and osseous Bankart lesions,
respectively .
Compression deformities of the posterolateral humeral head are common,
occurring due to wedging of the soft cancellous bone of the humeral head under the hard compact bone of the glenoid rim,
referred as “Hill-Sachs lesion” [4].
The primary criterion for surgery following anterior shoulder dislocation is the degree of risk of recurrent instability.
Causes of continued instability include Bankart and bony Bankart lesions (Fig.7),
a large Hill-Sachs lesion,
rotator cuff tear,
and tear of the capsular glenohumeral ligaments [5,6].
The measuring of the area of glenoid fossa bone loss can helps the surgeon determine the need for surgical repair of a bony Bankart lesion.
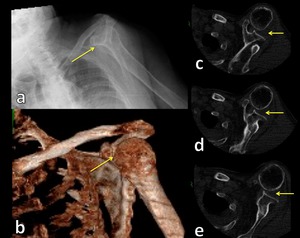
Fig. 5: Radiograph (a), 3D CT image (b) and axial CT images (c,d,e) show anterior glenohumeral dislocation.
References: Institute of Radiology, Catholic University - Rome/IT
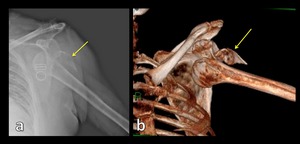
Fig. 6: Radiograph (a) and 3D CT image (b) show anterior glenohumeral dislocation with a displacement of humeral greater tuberosity
References: Institute of Radiology, Catholic University - Rome/IT
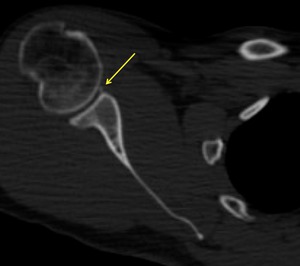
Fig. 7: Axial CT image show bony Bankart lesion (yellow arrow).
References: Institute of Radiology, Catholic University - Rome/IT
POSTERIOR GLENOHUMERAL DISLOCATION
Posterior glenohumeral dislocation is a rare type of shoulder dislocation (Fig.8).
Multiple mechanisms have been implicated in posterior shoulder dislocation,
most notably that of axial loading of the arm while adducted,
flexed,
and internally rotated; posterior dislocation less commonly results from a direct impact to the anterior aspect of the shoulder.
Posterior dislocations are most commonly classified according to postdislocation humeral head position:
- subacromial (most common)
- subglenoid
- subspinous
Traumatic posterior dislocations are commonly associated with a characteristic compression deformity of the anteromedial humeral head,
thought to be due to wedging of the humeral head against the posterior glenoid rim during subluxation,
termed a “reverse Hill-Sachs lesion”. Reverse Hill Sachs lesions are graded as small,
medium,
or large if the defect comprises up to 25%,
> 25–50%,
or greater than 50% of the articular surface,
respectively (Fig.9).
A posterior labral tear and posterior glenoid rim fracture have been termed soft-tissue and osseous “reverse Bankart lesions,” respectively.
The size of the humeral head defect therefore plays a role in determining the surgical approach.
Small defects can be treated with closed or open reduction; medium-sized defects can be repaired with fixation over the defect,
whereas large defects often require hemiarthroplasty.The primary significance of posterior dislocation is that it is frequently missed at clinical and radiologic examination,
resulting in a delay in diagnosis [7]. A chronic posterior dislocation is considered to be any dislocation that is diagnosed more than 3 weeks after the trauma.
Radiographic diagnosis of a posterior dislocation can be problematic but multiple signs have been reported to improve detection:
- Light bulb sign : refers to the appearance of the proximal humerus with the arm locked in internal rotation .
- Trough sign and rim sign: may also be seen on frontal radiographs,
although the humeral head defect and posterior dislocation are best seen on axillary radiograph views.
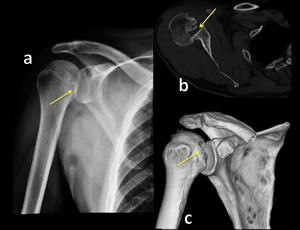
Fig. 8: Radiograph (a), axial CT scan (b) and 3D-CT image show posterior glenohumeral subluxation.
References: Institute of Radiology, Catholic University - Rome/IT
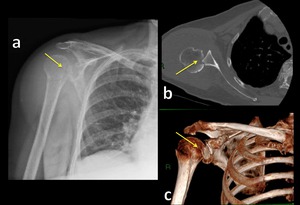
Fig. 9: Radiograph (a), axial CT scan (b) and 3D-CT image show posterior glenohumeral subluxation and reverse Hill-Sachs lesion (b, yellow arrow).
References: Institute of Radiology, Catholic University - Rome/IT
INFERIOR GLENOHUMERAL DISLOCATION
Traumatic inferior glenohumeral dislocations is a rare type of shoulder dislocation.
Inferior dislocation is most commonly seen due to falling onto an outstretched and abducted arm; direct axial loading with the arm hyperabducted is a less common alternate mechanism.
There is high incidence of associated bony and soft-tissue injuries,
including Bankart and Hill-Sachs lesions,
greater tuberosity fractures significant rotator cuff tears,
and brachial plexus injuries.
Surgical repair of Bankart and Hill-Sachs lesions and greater tuberosity fractures can be performed as indicated if instability is present.
Radiography is often adequate for initial evaluation of inferior dislocations.
CT can evaluate and characterize underlying osseous Bankart or Hill-Sachs lesions.
PROXIMAL HUMERUS FRACTURES
The Neer classification of proximal humeral fractures is the most used along with the AO classification of proximal humeral fractures (Fig.10,11,12,13,14).
The Neer classification system is based on the anatomic structures involved,
and fractures at one or more locations can result in division of the proximal humerus into as many as four parts:
- anatomic head
- lesser tuberosity
- greater tuberosity
- humeral shaft.
A part is considered to be separate only if it is displaced at least 1 cm or angled at least 45° [8].
Most fractures are one-part fractures,
which are generally treated nonsurgically.
Two-part fractures may require surgical repair,
and three- and four-part fractures may require surgical repair or shoulder arthroplasty [9].
The Neer classification system for proximal humerus fractures has a significant impact on treatment.
The radiologist must learn to describe the injury and provide measurements [10]:
- measurement of displacement (≥1 cm)
- measurement of angulation (≥45°)
- presence of articular split
- presence of anatomic neck fracture or fractures of both the lesser and greater tuberosities
- if anatomic neck is fractured,
length and displacement of medial metaphyseal segment
- presence of segmental surgical neck fracture
- presence of concomitant glenohumeral dislocation
The AO classification divides proximal humeral fractures into three groups,
A,
B and C,
each with subgroups,
and places more emphasis on the blood supply to the articular surface. The risk of avascular necrosis increases from type A (very low) to type C (high risk) and thus determines treatment.
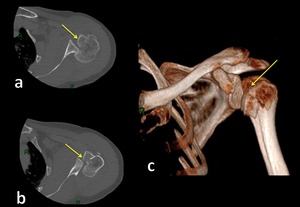
Fig. 11: Axial-CT (a,b) and 3D-CT image (c) show multifragment fracture of humeral head and posterior glenohumeral subluxation.
References: Institute of Radiology, Catholic University - Rome/IT
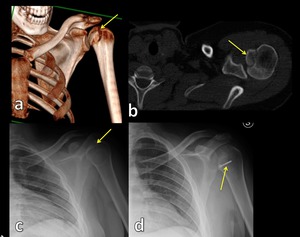
Fig. 10: 3D-CT image (a), axial CT scan (b) and radiograph view (c) show fracture/avulsion of lasser tubercle treated with surgical fixation (d), Hill-Sachs lesion and posterior glenohumeral subluxation.
References: Institute of Radiology, Catholic University - Rome/IT
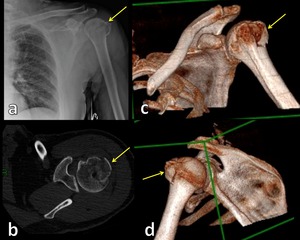
Fig. 12: Radiograph view (a), axial CT scan (b) and 3D-CT images (c,d) show multifragment fracture of humeral greater tuberosity.
References: Institute of Radiology, Catholic University - Rome/IT
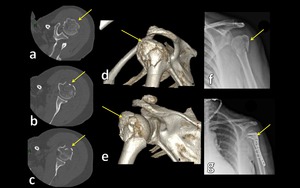
Fig. 13: Axial CT images (a,b,c), 3D-CT images (c,d) and radiograph (f) show multifragment fracture of proximal humerus.
References: Institute of Radiology, Catholic University - Rome/IT
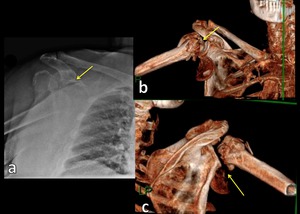
Fig. 14: Radiograph (a) and 3D-CT images (b,c) show multifragment fracture of proximal humerus and inferior dislocation of humeral head.
References: Institute of Radiology, Catholic University - Rome/IT

 and axial CT scan (c) show intraarticular fracture of the glenoid fossa treated with surgical fixation (d).
References: Institute of Radiology, Catholic University - Rome/IT")
, 3D CT image (b) and axial CT images (c,d,e) show anterior glenohumeral dislocation.
References: Institute of Radiology, Catholic University - Rome/IT")
 and 3D CT image (b) show anterior glenohumeral dislocation with a displacement of humeral greater tuberosity References: Institute of Radiology, Catholic University - Rome/IT")
, axial CT scan (b) and 3D-CT image show posterior glenohumeral subluxation. References: Institute of Radiology, Catholic University - Rome/IT")
, axial CT scan (b) and 3D-CT image show posterior glenohumeral subluxation and reverse Hill-Sachs lesion (b, yellow arrow). References: Institute of Radiology, Catholic University - Rome/IT")
, axial CT scan (b) and radiograph view (c) show fracture/avulsion of lasser tubercle treated with surgical fixation (d), Hill-Sachs lesion and posterior glenohumeral subluxation. References: Institute of Radiology, Catholic University - Rome/IT")
 and 3D-CT image (c) show multifragment fracture of humeral head and posterior glenohumeral subluxation. References: Institute of Radiology, Catholic University - Rome/IT")
, axial CT scan (b) and 3D-CT images (c,d) show multifragment fracture of humeral greater tuberosity. References: Institute of Radiology, Catholic University - Rome/IT")
, 3D-CT images (c,d) and radiograph (f) show multifragment fracture of proximal humerus. References: Institute of Radiology, Catholic University - Rome/IT")
. References: Institute of Radiology, Catholic University - Rome/IT")
 and 3D-CT images (b,c) show multifragment fracture of proximal humerus and inferior dislocation of humeral head. References: Institute of Radiology, Catholic University - Rome/IT")