ECR 2016 / C-1653
Traumatic Shoulder Injuries: What Orthopedics want to know and Radiologists must learn to describe.
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2016
Poster Number:
C-1653
Type:
Educational Exhibit
Keywords:
Trauma, Diagnostic procedure, CT, Conventional radiography, Musculoskeletal joint, Education and training
Authors:
E. Federici, C. Dell'atti, V. Martinelli, M. Bartocci, D. Beomonte Zobel, N. Magarelli, L. Bonomo; Rome/IT
DOI:
10.1594/ecr2016/C-1653

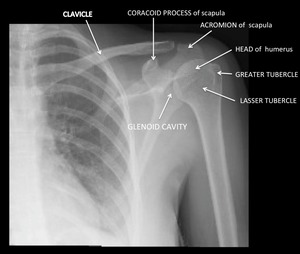
Fig. 1:
Normal radiographic anatomy of the proximal humerus and lateral scapula
 and external (b) rotation. Axillary lateral view (c) and transthoracic lateral view (d). References: Institute of Radiology, Catholic University - Rome/IT")
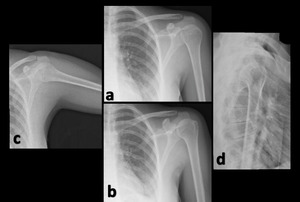
Fig. 2:
Anteroposterior radiographs in internal (a) and external (b) rotation. Axillary...
 image of the shoulder. References: Institute of Radiology, Catholic University - Rome/IT")
Fig. 3:
3D computed tomography (CT) image of the shoulder.