|
MRI Protocol - Benign Myometrial Pathology
|
In our service,
it is performed routinely the following protocol for suspected or follow-up of benign lesions of the myometrium:
Pelvis Sequences
- Axial T1 ( 5mm)
- Axial T2 ( 5mm)
Specific Sequences to the Uterus
- Sagittal T2 Body Uterus (4mm )
- Coronal T2 Body Uterus (4mm )
- Axial T2 Body Uterus (4mm )
Post Gadolinium Study
- Dynamic study - T1 * SPAIR – usually sagittal plane ( 5 purchases up to 150 sec.
) (2mm )
Normal 0 false false false PT JA X-NONE
- Late acquisition - T1 SPIR - usually sagittal and/or axial plane (4mm )
| Normal Myometrium - Anatomy |
- The uterus is divided into three layers — endometrium,
myometrium,
and serosa or perimetrium.
- The middle layer,
or myometrium,
is the muscular layer and it makes up most of the uterine volume.
- The myometrium is composed of mainly smooth muscle cells
- It can be separated into:
(1) the inner myometrium,
or junctional zone
(2) the outer myometrium.
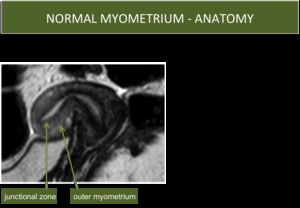
Fig. 1: Normal Myometrium Anatomy
- The junctional zone contains compact smooth muscle with little intercellular matrix,
and has a relatively low T2 signal intensity
- The outer myometrium has more intercellular matrix and vessels,
and less compact smooth muscle,
resulting in a higher T2 signal intensity.
- These T2 signal intensity differences are best visualized during the reproductive years (Fig.
1).
- T1-weighted images typically show poor contrast distinction between the endometrium and the myometrium.
- Benign tumours of myometrial origin
- The most common solid benign uterine neoplasm
- The most common tumors of the female genital tract (~25% of women of reproductive age)
- A number of factors are thought to contribute to leyomiomas development,
including genetic mutations and ethnicity
- Particularly common in the African population
- A major risk factor is exposure to unnopposed oestrogens:
*Obesity
*Early Menarche
*Late menopause
*Nulliparity
*Use of synthetic oestrogens (such as Tamoxifen in breast cancer treatment)
- As leiomyomas enlarge,
they may outhgrow their blood supply,
resulting in different types of degeneration:
*cystic degeneration
*hyaline or myxoid degeneration
*calcification
*hemorrhage (red degeneration)
Ultrasound
- Usually hypoechoic (but can be isooechoic or hyperechoic compared to normal myometrium)
- Calcification is seen as echogenic foci with shadowing
- Cystic areas of necrosis or degeneration may be seen
MRI
- T1
*non-degenerated fibroids and calcification appear as low to intermediate signal intensity compared with the normal myometrium
- T2
*non-degenerated fibroids and calcification appear as low signal intensity
*fibroids that have undergone cystic degeneration/necrosis can have a variable appearance,
usually appearing high signal on T2 sequences.
- T1 C+ (Gd)
*variable enhancement is seen with contrast administration
*marked high signal intensity with gradual enhancement suggests myxoid degeneration
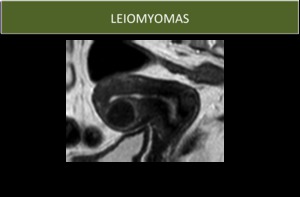
Fig. 3: Typical aspect of leyomioma on MRI.
LEIOMYOMA CLASSIFICATION
- Leiomyomas may be classified according to their location,
as:
*subserosal (beneath the serosa)
*intramural (within the substance of the myometrium)
*submucosal (projecting into the endometrial cavity) (Fig.
2)
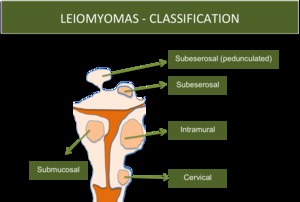
Fig. 2: Leiomyomas Classification
- Leiomyomas can involve the cervix (~8%),
mas most frequently occur in uterine corpus.
SYMPTOMS
- Commonly leiomyomas are an incidental finding and are asymptomatic
- 20-50% of leiomyomas are symptomatic
- symptoms are variable according to the size,
location and number os tumors
- The most common symptoms are menorrhagia,
dysmernorrhea,
pressure,
urinary freqyency,
pain,
infertility ou a palpable mass
CYSTIC DEGENERATION
- Represents ~ 4% of all types of degeneration
- Ultrasound shows a hypoechoic or heterogenous uterine mass with cystic areas
- MRI reveals a mass with portions of high T2 signal

Fig. 4: Leiomyoma with cystic degeneration
CALCIFICATION
- Seen in approximately 4% of fibroids
- Can be confined to the periphery of the fibroid, when it is thought to be secondary to thrombosed veins from previous red degeneration
- Calcific degeneration is difficult to distinguish from non-degenerated fibroids on MRI
- Areas of calcification can appear as signal voids on MRI

Fig. 5: Leiomyoma with calcification
MYXOIDE DEGENERATION
- Generally considered uncommon,
although reported as high a 50% by some authors
- They are filled with a gelatinous material
- It can be difficult to differentiate from fibroids that have undergone cysric degeneration
- They typically appear as complex cystic masses.
HYALINE DEGENERATION
- It occurs in up to 60% of uterine leiomyomas
- It happens when fibroids outgrow their blood supply
- As happens with calcifications, hyaline degeneration are difficult to distinguish from non-degenerated fibroids on MRI
- Amongst the background low T2 signal of non myxoid components,
there are areas of which typical characteristics include:
*T2: low signal
*T1 C+ (Gd): no enhancement
CARNEOUS DEGENERATION
- It is the most common form of degeneration of a leiomeyoma during pregnancy (it is a subtype of haemorrhagic infarction of leiomyomas that often occurs during pregnancy)
- Patients can present with abdominal pain (particularly during pregnancy),
fever and leucocytosis
MRI
Unusual signal intensity patterns have been described
- T1 :
*can have peripheral or diffuse high signal intensity
*the high signal intensity on T1-weighted images is likely secondary to the proteinaceous content of the blood or the T1-shortening effects of methemoglobin
- T2 :
*variable signal intensity with or without a low-signal-intensity rim.
*when it shows perihperal changes,
it may correspond with dilated vessels filled with red blood cells at the periphery of the lesion
- Rare benigne tumour if the uterus (incidence of 0.03-0.20%)
- Typically found primarily in obese perimenopausal and postmenopausal patients with typical uterine leiomyomas
- Most are asymptomatic
- Can cause symptoms similar to classic leiomyomas depending on their size and location (pelvic pain,
palpable mass and menstrual abnormalities)
- Etiology is not well known, but it is suggested that lipoleiomyomas result from fatty metamorphosis of uterine smooth muscle cells which can proceed to form localized or diffuse mature adipocyte tissue in leiomyoma or in the myometrium rather than fatty degeneration
- The tumor consists of long intersecting bundles of bland,
smooth muscle cells admixed with nests of mature fat cells and fibrous tissue.
- Main differential diagnosis: benign cystic teratoma, malignant degeneration of cystic teratoma,
non-teratomatous lipomatous ovarian tumor,
benign pelvic lipomas,
liposarcomas and lipoblastic lymphadenopathy.
- Ultrasound shows a hyperechoic mass with posterior accoustic attenuation
- On MRI:
- T1: hyperintensity
- T1 FS: hypointensity (saturates out)
- T2: hyperintensity
- T2 FS or STIR: hypointensity (saturates out)
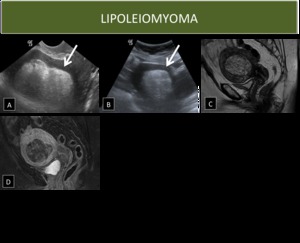
Fig. 6: Lipoleiomyoma
- IT can appear as a myometrial mass that has low signal intensity on T2W imaging and that bulges into the endometrial cavity
- The low signal intensity on T2W imaging is secondary to decreased water content in the area of contracted myometrium
- Diagnosis is easily made,
because myometrial contraction is a transient phenomenon and resolves on subsequent sequences
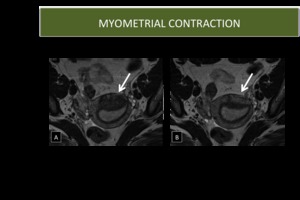
Fig. 7: Myometrial Contraction
| UTERINE ARTERIOVENOUS MALFORMATION |
- Can be congenital ou acquired
- Acquired UAVMs disease are associated with:
*multiple pregnancies
*miscarriage
*previous surgery (dilation and curettage,
termination of pregnancy or caesarean section)
Ultrasound:
- Areas of subtle myometrial inhomogeneity
- Tubular spaces within the myometrium
- A intramural uterine,
endometrial or cervical mass like region
- Prominent parametrial vessels
- Color Doppler shows serpiginous anechoic structures within the myometrium with a low resistance (RI ~0.2-0.5)
MRI:
- Multiple serpentine flow-related signal voids typically seen in the uterine wall,
endometrial cavity,
and parametrium on T1 and T2 weighted images
- Contrast-enhanced dynamic MR angiography shoes complex serpentine abnormal vessels that enhance as intensely as normal vessels and show early venous return

Fig. 8: Uterine Arteriovenous Malformation
- Defined by the presence of ectopic endometrial glands and stroma within the myometrium
- Typically affects women of reproductive age and multiparous
- More frequent in woman with a history of surgical uterine procedures (caesarian section,
dilatation and curettage)
- Typically present with menorrhagia and dysmenorrhea or chronic pelvic pain
- In 20% of cases is associated with endometriosis
Ultrasound
- Uterine enlargement
- Cystic anechoic spaces or lakes in the myometrium
- Uterine wall thickening (anteroposterior asymmetry)
- Subendometrial echogenic linear striations
- Heterogeneous echo texture
- Obscure endometrial/myometrial border
- Thickening of the transition zone (thickness of 12 mm or greater has been shown to be associated with adenomyosis)
MRI
- The most easily recognised feature is thickening of the junctional zone of the uterus to more than 12 mm (diffusely or focally)
- T2
* ill-defined region of thickening,
often with small high T2 signal regions representing small regions of cystic change
*may also have a striated appearance
- T1
*foci of high T1 signal are often seen,
indicating menstrual haemorrhage into the ectopic endometrial tissues
- T1 C+ (Gd)
*it is usually not indicated for evaluation of adenomyosis
*if performed,
it shows enhancement of the ectopic endometrial glands

Fig. 9: Adenomyosis
- Focal region of adenomyosis resulting in a mass
- It is difficult to distinguish from a leiomyoma
Ultrasound
- May be seen as a focal area of myometrical thickening
- It may also present as a heterogeneous focal nodule with indistinct margins and cystic spaces
MRI
- Localized,
low-signal-intensity region within the myometrium on both T2-weighted and contrast-enhanced T1-weighted sequences
- This region is often continuous with the junctional zone

Fig. 10: Adenomyoma
| DIFFERENTIAL DIAGNOSIS WITH OTHER THAN BENIGN MYOMETRIAL LESIONS |
LEIOMYOSARCOMA
- > 1/3 of uterine sarcomas but only 1.3% of all uterine cancers
- The uterus is the commonest location for a leiomyosarcoma
- Usually present in women in the 5th decade
- They are thought to arise de novo (incidence of sarcomatous transformation in benign uterine leiomyomas is reported to be 0.1-0.8%)
- Leiomyosarcomas are often difficult to differentiate from leiomyomas,
based on clinical features and even endometrial biopsy or dilatation and fractional curettage.
- Recent noinvasive or minimally invasive techiques in leiomyoma management have raised the importance of pretreatment imaging diagnosis of uterine sarcomas
- Generally larger and show more rapid growth than leiomyomas
MRI
- Uterus is often massively enlarged
- An irregular margin of a uterine leiomyoma on MRI is suggestive of sarcomatous transformation,
but this is not a specific signal!
- T1-weighted images: Large infiltrating myometrial mass of heterogeneous hypointensity with irregular and ill-defined margins
- T2-weighted images: intermediate-to-high signal intensity,
with central hyperintensity indicative of extensive necrosis (present in >50% of cases)
- Hemorrhage is common
- Foci of calcifications may be present
- After contrast administration: early heterogeneous enhancement,
due to the areas of necrosis and hemorrhage
Tips to Differential Diagnosis
The most suggestive features of malignancy are:
- Presence of irregular margins
- Necrosis
- Rapid growth

Fig. 11: Leiomyoma vc leiomyosarcoma

Fig. 12: Leiomyoma vc adnexal lesion

Fig. 13: Leiomyoma vc adnexal lesion
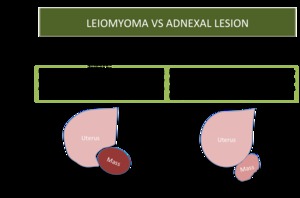
Fig. 14: Leiomyoma vc adnexal lesions

Fig. 16: Leiomyoma vc adnexal lesion
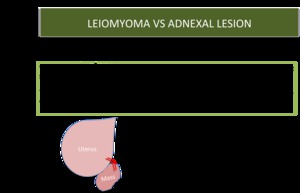
Fig. 17: Leiomyoma vc adnexal lesion

Fig. 18: Leiomyoma vc adnexal lesion

Fig. 15: Leiomyoma vc endometryal lesion


















