Femoroacetabular impingement
Clinical findings
Pain,
although unspecific,
has a major role in the diagnosis of FAI.
Without hip pain the diagnosis should not be made,
since radiographic signs of pincer or cam deformities are very prevalent in asymptomatic patients (67% and 37%,
respectively) and so they are clinically irrelevant.
3.
In patients who complaint of hip pain it is typically described as a deep,
diffused groin pain,
which exacerbates during flexion,
adduction or internal rotation.
This clinical syndrome is a common indication for further imaging investigation One major clinical finding is the "Dreahmann’s sign".
It describes unavoidable passive external rotation of the hip when performing hip flexion.
Although it is an unspecific sign,
it is often related with FAI.
Imaging findings
Conventional x-ray is the gold standard for early detection of FAI. Usually requires at least two radiographs,
one of the anteroposterior pelvic view and the axial cross table view (fig.
2) or Dunn/Rippstein view (fig.
3).
Occasionally a Faux profile (fig.
3) or a Lequesne view (fig.
4) can be accomplished to search for secondary changes of FAI.
Less frequently a Lowenstein/frog leg lateral view (fig.
4) can be performed.
Conventional imaging is also important to diagnose concomitant disorders and/or to exclude other pathologies such as rheumatoid arthritis and avascular necrosis (fig.
5).

Fig. 2: A:Anteroposterior pelvic view. B: Cross table view.
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.
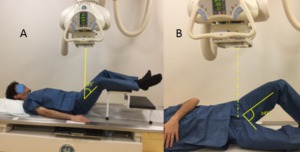
Fig. 3: A:Dunn/Rippstein view. B:Faux profile.
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.

Fig. 4: A: Lequesne view. B: Lowenstein or frog leg lateral view.
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.

Fig. 5: Male patient, 57 years old, with left hip pain. Left hip x-ray in an anteroposterior view demonstrates an increased sclerosis of the femoral head, with mottled and flattened appearance of the articular cortex (blue arrow), without any subchondral lucency - avascular necrosis of the hip - Ficat stage III.
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.
Pincer impingement
Pincer impingement hip osteoarthritis develops after repetitive microtrauma between the overgrown acetabular rim and the proximal femur with subsequent inflammatory and degenerative responses that will eventually lead to a thin (4 mm) circumferential chondral damage of adjoining articular cartilage.
It has a female predominance (M:F - 1:3) and usually appears within the average age range of 40 – 57 years old.
2 This acetabular overgrowth that hinders hip movement can be focal or general.
General acetabular overcoverage
In general acetabular overgrowth there is Pincer Coxa Profunda and Protrusio Acetabuli.
It is still not known if they are individual entities or a continuation of each other,
being protrusio acetabuli the more severe,
displaying stronger radiographic signs of a deeper femoral head.
A usual presenting sign of coxa profunda is the overlapping or crossing over of the fossa acetabular line over the ilioischial line (fig.
6),
while in protrusio acetabuli the femoral head additionally projects medial to the ilioischial line (fig.
7).

Fig. 6: Male patient, 52 years old, with left hip pain. Left hip x-ray in an anteroposterior view showing the fossa acetabular (F) overlapping the ilioischial line(IIL) typical of Pincer Coxa Profunda.
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.
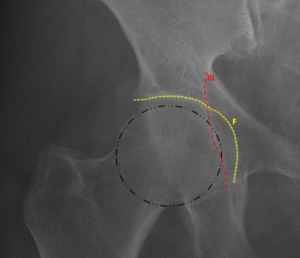
Fig. 7: Female patient, 46 years old, with right hip pain. Right hip x-ray in an anteroposterior view demonstrates the femoral head overlapping the ilioischial line(IIL) and a deeper fossa acetabular (F) that projects medial to the ilioischial line making it a typical case of Pincer Protrusio Acetabuli.
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.
The quantification of pincer severity (acetabular overcoverage) can be achieved by measuring the acetabular index (fig.8),
the lateral center edge angle (fig.
13) or the femoral head extrusion index (fig.
10).
The acetabular index also called “acetabular roof angle”,
is one method of acetabular over coverage quantification realized by measuring the angle formed by a horizontal line and a line connecting the medial point of the sclerotic zone with the edge of the acetabulum.
In normal hips the angle is usually positive (fig.
8),
but in those with coxa profunda it is usually neutral or only slightly positive (fig.
9 left hip).
In protusio acetabuli the angle can even be negative (fig.
9 right hip).
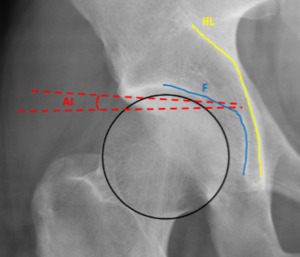
Fig. 8: Female patient, 31 years old, right hip x-ray in an anteroposterior view depicting a normal femoral head with a positive acetabular index (AI).
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.
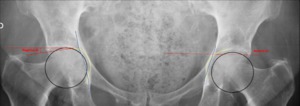
Fig. 9: Female patient, 43 years old, with bilateral hip pain, anteroposterior hip x-ray showing a protrusio acetabuli with a negative acetabular index (AI) on the right hip joint and a coxa profunda on the left joint with a neutral acetabular index(AI).
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.
The femoral head extrusion index is another method for quantification of acetabular overcoverage,
where the percentage of uncovered femoral head can be calculated.
A normal head extrusion index is under 25% (fig.
10).
Higher values are common in hip dysplasia (fig.
12) while pincer hips will have an index lower than 10% (fig.
11).
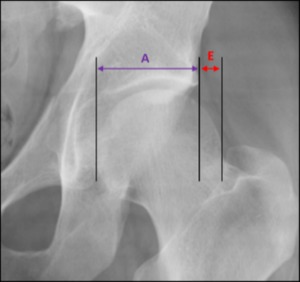
Fig. 10: Male patient, 31 years old, left hip x-ray in an anteroposterior view depicting a normal femoral head extrusion index: E/(E+A))x100 ≤ 25%.
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.
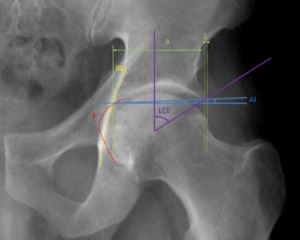
Fig. 11: Male patient, 52 years old, left hip x-ray in an anteroposterior view depicting a fossa acetabular (F) overlapping the ilioischial line, typical of a coxa profunda that can be quantified with a decreased femoral head extrusion index ( E/(E+A))x100 ≤ 10% )and an increased lateral center edge angle ≥ 39º.
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.
Yet another quantification method of the acetabular overcoverage is the lateral center edge (“wiberg angle"),
measured by the angle formed by two lines across the femoral head center,
one vertical line and another connecting the edge of the acetabulum (fig.
13).
The normal lateral center edge range of values goes from 25º that defines dysplasia (fig.
12) to 39º that defines pincer overcoverage (fig.
11 and 14).
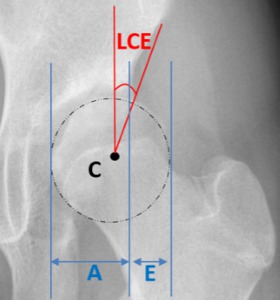
Fig. 12: : Female patient, 43 years old, left hip x-ray in an anteroposterior view depicting a widened joint space specially in the inferior articular portion, due to a mild lateral and superior displacement of the femoral head associated with a lateral center edge under 25º and an increased femoral head extrusion index: E/(E+A)x100≥25% typical of hip dysplasia.
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.
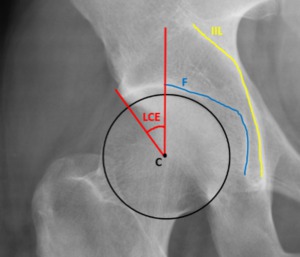
Fig. 13: Female patient, 31 years old, right hip x-ray in an anteroposterior view depicting a normal lateral center edge angle between 25º and 39º.
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.
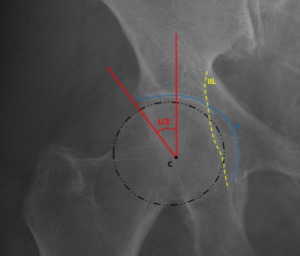
Fig. 14: Female patient, 46 years old, with bilateral hip pain. Right hip x-ray in an anteroposterior view demonstrates a femoral head that overlaps the ilioischial line(IIL), with an even deeper fossa acetabular (F) that’s medial to the ilioischial line, and displaying a lateral center edge angle (LCE) over 39º typical of pincer protrusio acetabuli.
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.
Focal acetabular overcoverage
Focal femoral head overcoverage can occur in the anterior or the posterior part of the acetabulum.
Posterior acetabular focal overcoverage happens when the posterior wall line passes laterally to the femoral head center,
depicting a more prominent posterior wall and eliciting the “posterior wall” sign (fig.
15).
It is common to have an association between a prominent posterior wall and pincer impingement.2
This posterior type of impingement can be responsible for hip pain during triggered by hip extension and external rotation.
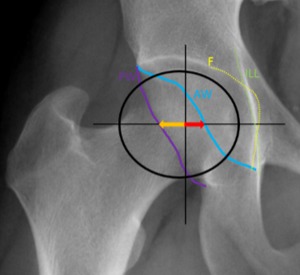
Fig. 15: Male patient, 62 years old, with right hip pain. Right hip x-ray in an anteroposterior view demonstrates the “posterior wall sign” with a too prominent posterior wall depicted by the orange arrow (longer than the red arrow). Since the posterior wall is laterally placed over the femoral head center, these aspects are typical of a focal overcoverage pincer. We can also view a coxa profunda since the acetabular fossa (F) overlaps the ilioischial line(IIL).
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.
Anterior acetabular overcoverage,
also called “cranial acetabular retroversion” or “anterior focal acetabular retroversion” is a focal type of pincer impingement due to a prominent anterior acetabular wall that is placed outermost relative to the posterior wall creating a cross-over sign or a "figure 8 sign" (fig.
16).
A deficient posterior wall can also reveal dysplasia (fig.
12) and acetabular retroversion.
Patients displaying this type of focal pincer FAI have symptoms during flexion and internal rotation of the hip due to chondral damage mainly in the posteroinferior part of the acetabulum.
This is called a countercoup lesion,
is a bad prognostic sign and is usually seen in the faux profile3 (fig.
17).
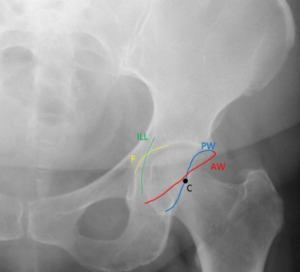
Fig. 16: Male patient, 65 years old, with left hip pain. Left hip x-ray in an anteroposterior view demonstrates the “cross-over sign” or “figure 8 sign” with a laterally placed anterior wall(AW) and a commonly placed posterior wall centered in the femoral head (C). These aspects are typical of a focal anterior overcoverage pincer / acetabular retroversion.
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.
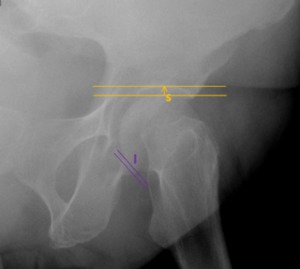
Fig. 17: Faux profile of the same patient of fig. 16. The focal anterior wall acetabular overcoverage is making the femoroacetabular head retroverted, with decreasing posteroinferior joint space (I), an unfavorable prognostic sign.
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.
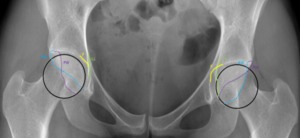
Fig. 18: Female patient, 33 years old, with bilateral hip pain. Hip x-ray in an anteroposterior view demonstrates the “cross-over sign” or “figure 8 sign” in both joints, with a laterally placed anterior wall (AW) and a typically placed posterior wall on the right joint, centered in the femoral head. Deficient posterior wall (PW) on the left hip joint being medially placed over the femoral head center. These aspects are typical of a focal anterior overcoverage pincer as an acetabular retroversion.
Also due to the fact that the ilioischial line is more lateral than the acetabular fossa on the right joint and it overlaps the femoral head on the left joint, these findings are suggestive of a pincer coxa profunda on the right hip and protusio acetabuli on the left hip.
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.
In cases of Pincer impingement we should consider the presence of associated disorders,
such as:
- Bladder extrophy
- Proximal femoral focal deficiency
- Posttraumatic dysplasia
- Chronic residual dysplasia of acetabulum
- Legg-Calvé-Perthes disease
- Slipped capital femoral epiphysis after acetabular reorientation procedures
- Idiopathic retroversion
Cam impingement
Cam impingement has a male predominance (M:F - 14:1).
It usually appears between 21 to 51 years old and has an average depth of cartilage damage of 11 mm,
in contrast to pincer that usually only affects 4 mm.2 In cam impingement,
early osteoarthritis develops after repetitive microtrauma between the acetabular rim and the nonspherical femoral head,
with subsequent inflammatory and degenerative responses that will eventually lead to an inflammatory process that will take to reactive ossification mostly on the labrum,
labrum tears,
cartilage damage and ultimately premature osteoarthritis.
This head asphericity is due to an osseous bump formation on the head and neck-junction.
If the osseous formation is anteroposterior it depicts a characteristic “pistol grip sign" in anteroposterior hip radiograms (fig.
19).
If the osseous extrusion is anterosuperior it’s best viewed in axial views (fig.
21).
Quantification of asphericity can be accomplished by measuring the angle α,
the femoral head neck offset and the femoral head neck offset ratio.
Femoral head neck offset is defined by the distance between a horizontal line over the widest portion of the femoral head and another horizontal line in the widest portion of the femoral neck.
In cam impingement the offset is reduced due to the osseous bump that leads to a higher line over the femoral neck.
Anterior offset values under 1 cm are a strong indicator of cam impingement (fig.
21).
The femoral head offset ratio is calculated by dividing the anterior offset by the diameter of the femoral and it is between 0,21±0.03 in asymptomatic patients (fig.
20) and 0.13±0.05 in hips with cam impingement (fig.
21).2 The angle α is measured by the angle formed between the femoral neck axis and a line connecting the head center with the point of beginning of asphericity,
a normal α is under 50 º,
while cam impingement will display a α≥50º (fig.
21).

Fig. 19: Male patient, 53 years old, with hindered hip mobility. Hip x-ray in an anteroposterior view demonstrates the cam “pistol grip sign” bilaterally(red lines). Since the acetabular fossa overlaps the ilioischial line we are faced with a mixed general overcoverage acetabular pincer and a cam type of femoroacetabular impingement. We can also view an acetabulary roof cyst bilaterally (arrows), a usual secondary radiographic sign of femoroacetabular impingement.
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.
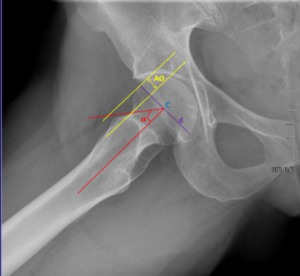
Fig. 20: Male patient, 33 years old, Hip x-ray in an axial Dunn/Rippstein view shows the normal α ≥50º, an normal anterior offset(AO) ≥ 1 cm and a normal femoral head offset ratio AO/d=0.21 ± 0.03.
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.
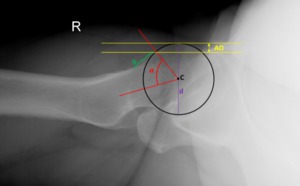
Fig. 21: Male patient, 33 years old, with right hip pain. Hip x-ray in an axial cross table view depicting an osseous bump in the anterior-superior portion of the femoral head-neck junction (b), eliciting an α ≥50 º, a decreased femoral anterior offset(AO) ≤ 1 cm and a femoral head offset ratio AO/d=0,13 ± 0,05, typical of Cam FAI.
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.
Another cause of cam impingement is femoral retrotorsion,
only reliably calculated when using CT scans.
Coxavara has already been reported as a predisposing factor for cam impingement2 and it can be identified by measuring central columdiaphysial angle under 125º.
A combination of both cam and pincer is present in as many as 86% of the affected patients.2
In cases of Cam impingement we should consider the presence of associated disorders,
such as:
- Slipped capital femoral epiphysis
- Legg-Calvé-Perthes disease
- Posttraumatic retrotorsion of femoral head
- Coxa vara
- Pistol-grip deformity
- Head-tilt deformity
- Post-slip deformity
- Femoral retroversion
- Growth abnormality of femoral epiphysis
Secondary radiographic changes due to femoroacetabular impingement
“Os acetabulum” is an acetabular rim fracture due to stress,
made by femoroacetabular impingement over repetitive trauma .
“Os acetabulum” is not present at an early stage of the femoroacetabular impingement pathology but rather presents itself later on,
and increases the disease progression by further deepening the femoral head and increasing the impingement problem.
(fig.
22 and 23)
Herniation pits are benign radiolucencies,
ranging from 3 mm to 15 mm,
surrounded by a sclerotic margin typically located in the femoral head and neck.
Although an incidental finding,
they occur in one third of patients with femoroacetabular impingement but are not associated with the disease progression or severity (fig.
22 and 23).
Another radiolucency that depicts secondary changes of FAI are the acetabulary roof cysts (fig.19).
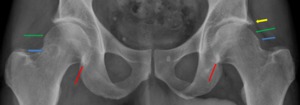
Fig. 22: Male patient, 68 years old, with right hip pain. Hip x-ray in an anteroposterior view demonstrates an osseous bump in femoral head-neck junction typical of cam pistol grip impingement (green arrows). There are secondary radiographic changes due to femoroacetabular impingement as: herniation pits depicted as a radiolucency evolved by a sclerotic margin ( blue arrows); posteroinferior sclerosis with joint space narrowing, which is an unfavorable prognostic sign (best viewed in a faux profile)(red arrows); and a left “os acetabuli” due to an acetabular rim fracture after repetitive trauma of the femoral head against the acetabulum (yellow arrow).
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.

Fig. 23: Female patient,42 years old, with left hip pain. Hip x-ray in an anteroposterior view demonstrates an overlap of the lateral ilioischial line over a more medial acetabular fossa, typical of a pincer, general acetabular overcoverage coxa profunda. Some secondary radiographic changes can be seen: herniation pits depicted as a radiolucencies evolved by a sclerotic margin ( blue arrows); a left “os acetabuli” due to an acetabular rim fracture after repetitive trauma of the femoral head against the acetabulum (green arrow).
References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.
Posteroinferior joint space narrowing due to recurrent subluxations and femoroacetabular impingement disease progression is an unfavorable prognostic finding of increased hip osteoarthritis,
with the need for total hip replacement.
This unfavorable sign is best illustrated in a faux profile (fig.
17).
Crossed sectional imaging
CT scans permit measuring centrum columndiaphyseal angles,
which permit identification of a coxa vara type of cam femoroacetabular impingement.
CT studies also allow for a more accurate evaluation of the bone structures and an accurate evaluation of calcific metaplasia of labrum,
scarcely detectable using MR.
Conversely,
MRI allows for a more precise evaluation of subcortical bone damage,
since simple MRI evaluation allows for a limited analysis of labrum and of the cartilage-labrum complex.
In this setting,
MRI arthrography is considered the gold standard.
This technique uses the intra-articular injection of a gadolinium-based contrast agent to elicit capsular distension,
allowing evaluation with improved detail.
Albeit newer radiographic technics,
conventional imaging is still the gold standard for initial assessment of femoroacetabular impingement.
Treatment
It is still unclear when to act surgically.
A wise and conscious approach is of paramount importance.
Cessation of extreme sports that elicit repetitive trauma in extreme angles jamming the femoral head against the acetabulum is obvious.
Drugs and physiotherapy are not viable options,
leaving only,
to those in need,
a surgical approach.
The scientific community has yet to find its route.
Nevertheless it seems that arthroscopy is gaining followers.
Although it is still harder to perform than open surgery,
its minimalistic approach with fewer complications and fast recovery makes it an usual first choice for surgically treated patients.
Mini open surgery remains as a mixed form of the former two having both types of open surgery and arthroscopy.
For those in whom the disease is already advanced there’s no other option than total hip replacement with hip prosthesis.
Long-term studies on this topic are still missing.





, without any subchondral lucency - avascular necrosis of the hip - Ficat stage III. References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.")
 overlapping the ilioischial line(IIL) typical of Pincer Coxa Profunda. References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.")
 and a deeper fossa acetabular (F) that projects medial to the ilioischial line making it a typical case of Pincer Protrusio Acetabuli. References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.")
. References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.")
 on the right hip joint and a coxa profunda on the left joint with a neutral acetabular index(AI). References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.")
)x100 ≤ 25%. References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.")
 overlapping the ilioischial line, typical of a coxa profunda that can be quantified with a decreased femoral head extrusion index ( E/(E+A))x100 ≤ 10% )and an increased lateral center edge angle ≥ 39º. References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.")
x100≥25% typical of hip dysplasia. References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.")

, with an even deeper fossa acetabular (F) that’s medial to the ilioischial line, and displaying a lateral center edge angle (LCE) over 39º typical of pincer protrusio acetabuli. References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.")
. Since the posterior wall is laterally placed over the femoral head center, these aspects are typical of a focal overcoverage pincer. We can also view a coxa profunda since the acetabular fossa (F) overlaps the ilioischial line(IIL). References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.")
 and a commonly placed posterior wall centered in the femoral head (C). These aspects are typical of a focal anterior overcoverage pincer / acetabular retroversion. References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.")
, an unfavorable prognostic sign. References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.")
 and a typically placed posterior wall on the right joint, centered in the femoral head. Deficient posterior wall (PW) on the left hip joint being medially placed over the femoral head center. These aspects are typical of a focal anterior overcoverage pincer as an acetabular retroversion.
Also due to the fact that the ilioischial line is more lateral than the acetabular fossa on the right joint and it overlaps the femoral head on the left joint, these findings are suggestive of a pincer coxa profunda on the right hip and protusio acetabuli on the left hip. References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.")
. Since the acetabular fossa overlaps the ilioischial line we are faced with a mixed general overcoverage acetabular pincer and a cam type of femoroacetabular impingement. We can also view an acetabulary roof cyst bilaterally (arrows), a usual secondary radiographic sign of femoroacetabular impingement. References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.")
 ≥ 1 cm and a normal femoral head offset ratio AO/d=0.21 ± 0.03. References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.")
, eliciting an α ≥50 º, a decreased femoral anterior offset(AO) ≤ 1 cm and a femoral head offset ratio AO/d=0,13 ± 0,05, typical of Cam FAI. References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.")
. There are secondary radiographic changes due to femoroacetabular impingement as: herniation pits depicted as a radiolucency evolved by a sclerotic margin ( blue arrows); posteroinferior sclerosis with joint space narrowing, which is an unfavorable prognostic sign (best viewed in a faux profile)(red arrows); and a left “os acetabuli” due to an acetabular rim fracture after repetitive trauma of the femoral head against the acetabulum (yellow arrow). References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.")
; a left “os acetabuli” due to an acetabular rim fracture after repetitive trauma of the femoral head against the acetabulum (green arrow). References: Department of Radiology, Centro Hospitalar de Lisboa Central, Lisboa, Portugal.")