Target Population:
Paediatric head,
chest and abdomen CT examinations,
performed in a radiology department from a public hospital.
Study Type
1.
Retrospective study (probabilistic sample);
2.
Quantitative study (experimental method using two phantoms)
Variables:
Independent variables: Baseline current-time product (mAs) and protocol parameters: tube voltage (kVp),
current-time product (mAs),
pitch.
.
Dependent variables: CTDIvol values (Volume Computed Tomography Dose Index),
DLP values (Dose-length product),
CT image quality parameters (noise,
low contrast resolution,
high contrast resolution),
reduction factor and appropriate paediatric mAs.
Instruments
Protocol for dose reduction in paediatric CT examinations (Table 1 and Table 2);
Cardinal Health phantom (model 76-415);
Gammex 464 phantom;
16 slices CT equipment;
CTDI ionization chamber;
Electrometer;
Medical Application DICOM viewer/server;
Microsoft Excel.
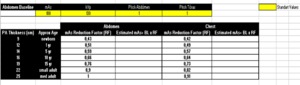
Table 1: mAs Reduction Factor for the Paediatric Abdomen and Chest CT
References: Medical Imaging and Radiotherapy Department, Health School - University of Algarve, Portugal.
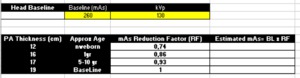
Table 2: mAs Reduction Factors for the Paediatric Head CT
References: Medical Imaging and Radiotherapy Department, Health School - University of Algarve, Portugal.
Procedures:
1. Retrospective study
Data from paediatric head,
chest and abdomen CT examinations (performed between January 2014 and April 2015) were recorded for determination of technical exposure parameters (mAs,
kVp,
pitch) and doses (CTDIvol,
DLP) applied by the radiographers in the radiology department under study.
It was obtained a sample of 85 head,
12 chest and 9 abdomen examinations.
Data were recorded in Excel tables and then the mAs average values were calculated according the age group.
In this research it was found that CT equipment doesn’t have predefined protocols optimized for paediatric patients,
so the standard protocol for adult is used as reference for paediatric examinations and the radiographers adjust the tecnhical parameters.
The average values of current-time product (mAs) used by radiographers in paediatric head CT examinations by age group (newborn,
1 year,
5years and 10 years) are showed in table 3.
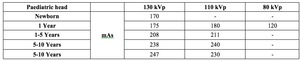
Table 3: Protocols used by Radiographers in paediatric head CT examinations
References: Medical Imaging and Radiotherapy Department, Health School - University of Algarve, Portugal.
It is not allowed to make the same kind of evaluation for abdomen and chest examinations because it was used a small sample.
2.
Quantitative study
2.1.
Quality control of the CT equipment
Quality control of the equipment was made using a Cardinal Health phantom (model 76-415) (Fig.1).

Fig. 1: Quality control of the CT equipment made using a Cardinal Health phantom (model 76-415) and the ionization chamber
References: Medical Imaging and Radiotherapy Department, Health School - University of Algarve, Portugal.
The CT equipment calibration were performed by means of the correlation between the CTDIvol obtained with the ionization chamber positioned within the phantoms,
considering the acquisition of a section at the central position of the chamber,
and the CTDIvol provided by the equipment.
The CTDIvol is obtained from the ratio between the weighted computed tomography dose index (CTDIw) and the pitch.
When the index of correlation between the values obtained in the measurements performed with the ionization chamber and those provided by the equipment is approximately 100% it means that the equipment is calibrated.
2.2. Determination of the appropriate mAs for a paediatric chest abdomen and head CT and the dose values obtained
As suggested by Society for Paediatric Radiology (2007),
baseline technical parameters for the adult abdomen and head were recorded.
Then,
to determine the appropriate mAs for paediatrics examinations,
baseline mAs was multiplied by the indicated Reduction Factor and the other technical parameters in protocol (kVp,
pitch) remained the same.
In this step,
the adapted protocols were defined,
exposures were made in a Gammex 464 phantom and the dose values obtained were recorded.
When comparing the average values of current-time product used by radiographers in paediatric head CT examination with the values estimated in the protocol (Table 4),
it is possible concluded that Radiographers use lower current-time products than suggested. So,
it was decided (by a Physical medical specialist) to apply the proposed protocol on the protocol of radiographers and,
after the analysis of image quality,
determine how much is possible and acceptable to reduce the dose.
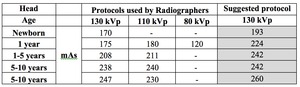
Table 4: Head paediatric CT protocols
References: Medical Imaging and Radiotherapy Department, Health School - University of Algarve, Portugal.
The same procedure wasn’t made for the other anatomical regions due the low number of data,
so it was performed 7 exposures only (using the protocol suggested by the Society for Pediatric Radiology) for Abdomen/Chest.
In the tables 5 and 6 are established the technical exposure parameters (mAs and kVp) used and the CTDIvol and DLP values obtained for each of these protocols; it was assigned a number from 1 to 20,
in the table 5,
to head CT examinations,
and 1 to 7,
in the table 6,
to abdomen CT examinations.
In head exposures,
all technical exposure parameters was established using manual techniques but in the abdomen exposures it wasn’t possible,
so it was applied the automatic exposure control (AEC).
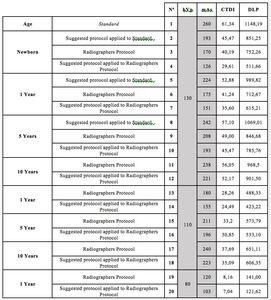
Table 5: Paediatric head CT protocols submitted to image quality control
References: Medical Imaging and Radiotherapy Department, Health School - University of Algarve, Portugal.
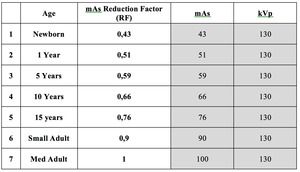
Table 6: Paediatric abdomen CT protocols submitted to image quality control
References: Medical Imaging and Radiotherapy Department, Health School - University of Algarve, Portugal.
2.3. Image Quality
To verify the image quality,
considering the American College of Radiology standards and using the determined exposure parameters with a reduction factor,
20 exposures were made in a Gammex 464 phantom (Fig.2) with head CT protocols and 7 exposures with abdominal CT protocols.

Fig. 2: Gammex 464 phantom
References: Medical Imaging and Radiotherapy Department, Health School - University of Algarve, Portugal.
Several scanner parameters were examined,
these include: CT number accuracy and slice thickness (module 1,
Fig.3); Low contrast resolution and the contrast-to-noise ratio.
(module 2,
Fig.4); CT number uniformity (module 3,
Fig.5); high contrast (spatial) resolution (module 4,
Fig.6).
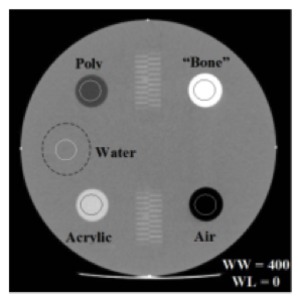
Fig. 3: Analyses of Phantom Gammex 464, Module 1
References: Medical Imaging and Radiotherapy Department, Health School - University of Algarve, Portugal.
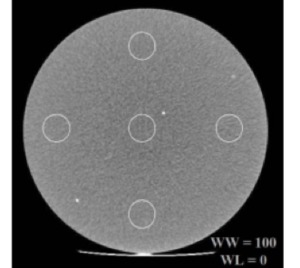
Fig. 4: Analyses of Phantom Gammex 464, Module 2
References: Medical Imaging and Radiotherapy Department, Health School - University of Algarve, Portugal.
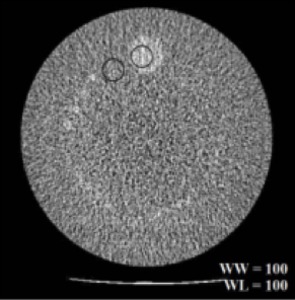
Fig. 5: Analyses of Phantom Gammex 464, Module 3
References: Medical Imaging and Radiotherapy Department, Health School - University of Algarve, Portugal.
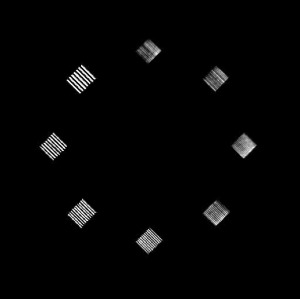
Fig. 6: Analyses of Phantom Gammex 464, Module 4
References: Medical Imaging and Radiotherapy Department, Health School - University of Algarve, Portugal.
