The reported prevalence of MDA varies widely in the literature,
ranging from 1%-5% in the general population to 13%-25% among women with recurrent pregnancy loss[1-3].
Clinically diagnosis of MDA is important because these are associated with primary amenorrhea,
infertility,
recurrent miscarriage,
obstretic complications and endometriosis.
It helps in identification of patients at risk of these complications and timely surgical intervention.
Fusion of the mullerian ducts normally occurs between the 6th and 11th weeks of gestation to form the uterus,
fallopian tubes,
cervix,
and proximal two-thirds of the vagina[4].
Any disruption to the fusion during this period results in spectrum of MDA.
MDA are also commonly associated with renal anomalies,
with a reported prevalence of 30%-50%,
including renal agenesis (most commonly unilateral agenesis),
ectopia,
hypoplasia,
fusion,
rotation,
and duplication[4-6].
Between 6th to 9th week absence of mullerian inhibiting factor promotes growth of paired mullerian ducts and regression of mesonephric ducts.
This is followed by migration and fusion of mullerian ducts.
Between 9 to 12 weeks there will be resorption of the intervening uterovaginal septum.

Fig. 1: Development of uterus
Interruption of growth of paired mullerian ducts --Aplasia/Hypoplasia of vagina/cervix/uterus
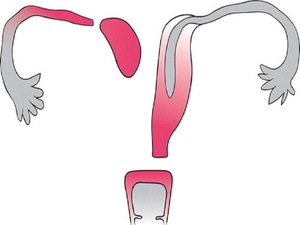
Fig. 2: Mullerian hypoplasia
References: Junqueira BLP, Allen LM, Spitzer RF, Lucco KL, Babyn PS, Doria AS. Müllerian Duct Anomalies and Mimics in Children and Adolescents: Correlative Intraoperative Assessment with Clinical Imaging. RadioGraphics [Internet]. 2009 Jul [cited 2016 Dec 15];29(4):1085–103. Available from: http://pubs.rsna.org/doi/10.1148/rg.294085737
Interruption of mullerian duct fusion -- Bicornuate uterus and Uterine didelphys

Fig. 3: Bicornuate uterus
References: Junqueira BLP, Allen LM, Spitzer RF, Lucco KL, Babyn PS, Doria AS. Müllerian Duct Anomalies and Mimics in Children and Adolescents: Correlative Intraoperative Assessment with Clinical Imaging. RadioGraphics [Internet]. 2009 Jul [cited 2016 Dec 15];29(4):1085–103. Available from: http://pubs.rsna.org/doi/10.1148/rg.294085737
Interruption of resorption -- Septate/ Arcuate uterus

Fig. 4: Septate uterus
References: Junqueira BLP, Allen LM, Spitzer RF, Lucco KL, Babyn PS, Doria AS. Müllerian Duct Anomalies and Mimics in Children and Adolescents: Correlative Intraoperative Assessment with Clinical Imaging. RadioGraphics [Internet]. 2009 Jul [cited 2016 Dec 15];29(4):1085–103. Available from: http://pubs.rsna.org/doi/10.1148/rg.294085737
Classification of MDA on the basis of American Society for Reproductive Medicine

Fig. 5: Classification of MDA
References: Joanna Culley, BA.
Both MRI and ultrasound can be utilized for imaging in patients suspected with MDA as they can be helpful in analyzing both cavity and contour of the uterus.
Ultrasound is the initial imaging of choice in female suspected with various pelvic pathologies due to its wide availability,
no ionizing radiation and cost effective.
While MRI is a useful option in the diagnosis of MDA,
with numerous studies having proved its excellent efficacy in this field[7-10].
3-dimensional ultrasound represents a valid alternative,
because,
in addition to its lower cost and better tolerance by patients,
it provides images of very similar quality to those yielded by MRI[11].
