Dynamic ultrasonography is performed with varying degrees of patient arm rotation and joint stress maneuvers.
Patient positioning must be comfortable for both the patient and operator.
Most authors prefer to scan facing the front of the patient rather than behind the patient.
Probe frequency selection depends on the patients build,
but a multifrequency linear transducer (9-12Mz) is usually appropriate for US shoulder evaluation.
Uncommonly a 9-MHz transducer is required for extremely large patients to allow depth penetration (with less resolution).
The basic objectives for each step are to identify the tendon of interest in two planes,
eliminate artifact (the most common relates to anisotropy) and diagnose disease.
A scanning protocol should include the following checklist of key structures:
- Long head of the biceps tendon
- Subscapularis tendon
- Supraspinatus tendon
- Rotator interval
- Acromioclavicular joint
- Subacromial impingement
- Infraspinatus and teres minor tendons
- Posterior glenohumeral joint recess
1.
LONG HEAD OF THE BICEPS TENDON
The long head of the biceps tendon (LHBBT) is usually the first structure to be examined,
followed by assessment of the tendons of the four rotator cuff muscles.
ANATOMY
The long head of biceps brachii tendon (LHBBT) arises from the supraglenoid tubercle of the scapula and from the superior glenoid labrum as a long tendon,
which runs into the joint cavity of the shoulder,
between the humeral head and the joint capsule.
Then it passes up along the bicipital groove.
The tendon is intra-articular but extrasynovial,
with a surrounding synovial-lined sheath that communicates with the glenohumeral joint and extends into the bicipital groove.
TECHNIQUE AND EVALUATION
The US assessment is performed with the arm in neutral position.
The patient must place his hand palm up on the lap,
with the elbow joint flexed at 90°.
The transducer is placed in the axial plane over the anterior humeral head and starts by searching for the biceps tendon in the groove (localized between small and large tuberosity of the humerus).
The long head of the biceps tendon appears as an ovalar hyperechoic structure within the groove and small amounts of fluid can normally be seen surrounding the tendon.
The mean value of normal tendon thickness is 4.3 mm,
but it may vary.
Then,
the transducer must be rotated 90° to obtained a longitudinal view – long axis of the LHBBT.
Both transverse and longitudinal views should evaluate the vertical part of the LHBBT up to the myotendinous junction.
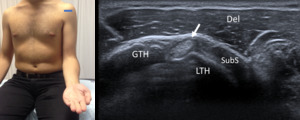
Fig. 1: Short axis of long head of the biceps tendon - Probe placement and US normal imaging findings. LTH, lesser tuberosity of the humerus; GTH, greater tuberosity of the humerus; Del, deltoid muscle; SubS, Subscapularis tendon; Arrow, long head of the biceps tendon
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
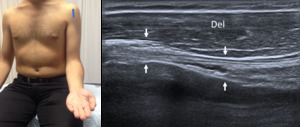
Fig. 2: Long axis of long head of the biceps tendon - Probe placement and US normal imaging findings. Del, deltoid muscle; Arrows, long head of the biceps tendon
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
The fibrillary pattern of the biceps tendon may appear hypoechoic in the longitudinal view due to probe angulation (anisotropy),
and usually is needed to pressing on the inferior aspect of the probe to ensure that the ultrasound beam is perpendicular to the biceps tendon.
These technical aspects will promote a homogeneous and normal echogenic fibrillar pattern and obtain better evaluation of the tendon.
2.
SUBSCAPULARIS TENDON
ANATOMY
The subscapularis muscle arises from the subscapular fossa.
The fibers run obliquely and laterally,
crossing the front of the glenohumeral joint and forming a tendon which inserts into the lesser tuberosity of the humerus.
TECHNIQUE AND EVALUATION
The patient must rotate the arm externally fixing the elbow on the iliac crest to visualize the subscapularis from its insertion into the lesser tuberosity to the point at which it becomes hidden by coracoid process medially.
The transducer is placed on the anterior shoulder,
approximately at the level of the coracoid process,
in a transverse orientation to scan the long-axis.
The transducer is then turned 90° to evaluate its short axis (sagittal plane).
The two planes must be evaluated during passive external and internal rotation,
with the arm adduced,
and the transducer must be moving superior and inferior to ensure a complete evaluation and the tendon integrity.
The hypoechoic subscapularis muscle,
which interdigitates with its multiple hyperechoic tendons,
or tendon anisotropy should not be misinterpreted as disease.

Fig. 3: Long axis of subscapularis tendon - Probe placement and US normal imaging findings. Del, deltoid muscle; LTH, Lesser tuberosity of the humerus; Arrows, subscapularis tendon.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT

Fig. 4: Short axis of subscapularis tendon - Probe placement and US normal imaging findings. Del, deltoid muscle; LTH, Lesser tuberosity of the humerus; Arrows, subscapularis tendon.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
3.
SUPRASPINATUS TENDON
ANATOMY
The supraspinatus tendon arises from the supraspinatous fossa and runs laterally under the acromial process and behind the clavicle lateral edge,
inserting on the most superior facet of the greater tubercle of the humerus.
TECHNIQUE AND EVALUATION
The patient´s arm must be posteriorly,
with flexed elbow and the palm side of the hand placed on the ipsilateral superior aspect of the iliac wing and directed toward the midline of the back.
In this position,
the supraspinatus rotates and becomes more anteriorly situated structure,
the acromion is moved away from the tendon and is visualized in its full extent.
The evaluation must be performed in two planes,
to visualize the tendon in long and short axis.
The greater tuberosity and the humeral head are very important bone landmarks during the supraspinatus tendon evaluation.
The thickness of the supraspinatus tendon varies from 6-6.5 mm,
measured at 2 cm proximally to its insertion on the greater tuberosity.
The long-axis view of the supraspinatus allows an accurate characterization of a tear (articular,
bursal,
intrasubstance,
or full-thickness).
The normal supraspinatus should be fibrillary and hyperechoic with a convex superior surface,
although some areas may appear hypoechoic due to anisotropy and the probe will need to be angled to avoid this artifact.
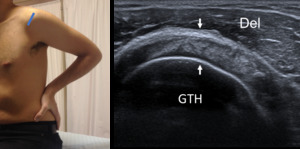
Fig. 5: Short axis of supraspinatus tendon - Probe placement and US normal imaging findings. Del, deltoid muscle; GTH, Greater tuberosity of the humerus; Arrows, supraspinatus tendon.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
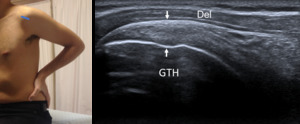
Fig. 6: Long axis of supraspinatus tendon - Probe placement and US normal imaging findings. Del, deltoid muscle; GTH, Greater tuberosity of the humerus; Arrows, supraspinatus tendon.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
4.
ROTATOR INTERVAL
ANATOMY
The rotator interval is a triangular anatomic area in the anterosuperior aspect of the shoulder,
which is defined by the coracoid process at its base,
superiorly by the anterior margin of the supraspinatus tendon,
and inferiorly by the superior margin of the subscapularis tendon.
It is roofed by the rotator interval capsule,
which is principally made up of the coracohumeral ligament.
It contains the tendon of the long head of the biceps and the superior glenohumeral ligament.
TECHNIQUE AND EVALUATION
The rotator interval is best evaluated with the arm in external rotation,
in the same position used in the evaluation of the supraspinatus.
The thin hyperechoic coracohumeral ligament can be identified superficial to the long head of the biceps tendon and the glenohumeral ligament is medial to the biceps tendon,
with a thin and hyperechoic appearance.
The combination of the coracohumeral ligament and superior glenohumeral ligament have a complex relationship which contributes to the biceps pulley,
acting together to hold the long head of the biceps from subluxing or dislocating anteriorly.
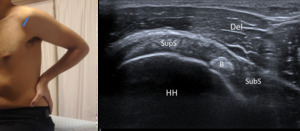
Fig. 7: Rotator Interval - Probe placement and US normal imaging findings. DM, deltoid muscle; B, Biceps tendon; HH, Humeral Head; Del, Deltoid muscle; SupS, Supraspinatus tendon; SubS, Subscapularis tendon.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
5.
ACROMIO-CLAVICULAR JOINT
ANATOMY
The acromio-clavicular joint is located between the acromio and clavicle.
TECHNIQUE AND EVALUATION
The acromio-clavicular joint is best evaluated when the transducer is oriented along the long axis of the clavicle with the patient´s arm in neutral position.
This view optimizes the visualization of the joint space,
synovium,
capsule,
and bonny margins of the joint.
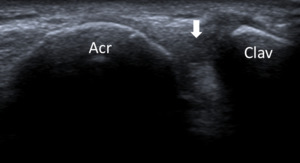
Fig. 8: Acromioclavicular joint - Probe placement and US normal imaging findings. Acr, acromion; Clav, clavicle; Arrow, acromio-clavicular joint space.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
6.
SUBACROMIAL IMPINGEMENT
ANATOMY
Subacromial impingement is a clinical syndrome that occurs secondary to attrition between the coracoacromial arch and the supraspinatus tendon or subacromial bursa.
TECHNIQUE AND EVALUATION
A dynamic assessment is fundamental to evaluate the subacromial impingement.
The probe is positioned with its medial margin at the lateral margin of the acromion,
in coronal oblique position,
viewing the greater tuberosity.
Then,
the patient must abduct and elevate his arm internally rotated.
During this maneuver,
the supraspinatus and the subacromial-subdeltoid bursa should slide smoothly under the acromion.
Fig. 9: Subacromial impingement – dynamic evaluation by ultrasonography.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
7.
INFRASPINATUS AND TERES MINOR TENDONS
ANATOMY
The infraspinatus muscle is a thick triangular muscle,
that arises from the medial part of the infraspinatous fossa (beneath the spine of the scapula) and runs laterally to insert on the middle facet of the greater tubercle of the humerus.
The teres minor arise just below the infraspinatus on the infraspinatous fossa and runs laterally to insert on the inferior facet of the greater tubercle of the humerus (and on the capsule of glenohumeral joint).
TECHNIQUE AND EVALUATION
The assessment must be realized by a posterior approach and the patient must have his elbow flexed and the palm place on the opposite shoulder (or his hand turned to the lap,
with palm up).
The spine of the scapula is as optimal landmark,
and the transducer must be placed just below the scapular spine in a slightly oblique axial plane,
producing a long-axis view of the infraspinatus tendon,
and following the tendon to it´s insertion postero-laterally on the humeral head.
In an inferior position,
we can find the teres minor below the infraspinatus.
The transducer is then rotated 90° to assess these tendons in short axis.
The infraspinatus tendon is larger and longer than the teres minor tendon.
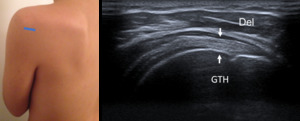
Fig. 10: Long axis of infraspinatus tendon - Probe placement and US normal imaging findings. Del, deltoid muscle; GTH, Greater tuberosity of the humerus; Arrows, infraspinatus tendon.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
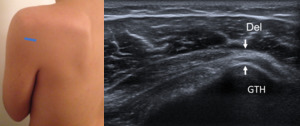
Fig. 11: Long axis of teres minor tendon - Probe placement and US normal imaging findings. Del, deltoid muscle; GTH, Greater tuberosity of the humerus; Arrows, teres minor tendon.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT

Fig. 12: Short axis of infraspinatus and teres minor muscles - Probe placement and US normal imaging findings. Del, deltoid muscle; InfraS, infraspinatus muscle; TM, teres minor muscle.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
8.
POSTERIOR GLENOHUMERAL JOINT RECESS
ANATOMY
The glenohumeral joint includes the margins of the labrum and glenoid rim to the anatomic neck of the humerus.
TECHNIQUE AND EVALUATION
To evaluate the posterior recess,
the transducer must slide medially on the posterior side of the joint while the patient´s arm is positioned in the same position used to evaluate infraspinatus and teres minor tendons.
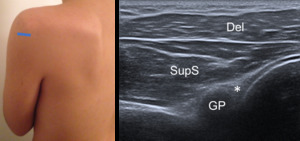
Fig. 13: Posterior glenohumeral joint recess - Probe placement and US normal imaging findings. Asterisk, posterior labrum; Del, deltoid muscle; SupS, Supraspinatus tendon; GP, glenoid process; HH, humeral head.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT












