ECR 2017 / C-2264
Neurosarcoidosis: A pictorial review.
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2017
Poster Number:
C-2264
Type:
Educational Exhibit
Keywords:
CNS, MR, Decision analysis, Tissue characterisation
Authors:
T. Buende Tchokouako, H. Nejadhamzeeigilani, J. L. Nix, I. Craven, D. J. Warren, J. Macmullen-Price, S. Currie; Leeds/UK
DOI:
10.1594/ecr2017/C-2264
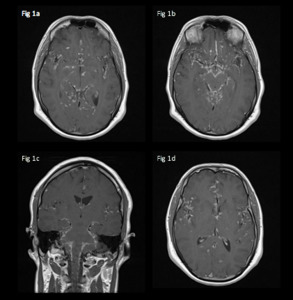
 and coronal (c) T1 post gadolinium show linear and nodular leptomeningeal thickening and enhancement predominantly at the base of the skull but also in the Sylvian fissures bilaterally, within the surface sulci and around the brainstem.")
Fig. 1:
24-year-old male admitted with headaches, nausea and fatigue.
Axial (a, b and...
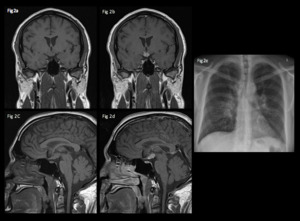
 and post (b, d) gadolinium show an enhancing mass in the infundibulum.
A chest radiograph (e) in the same patient shows bilateral hilar lymphadenopathy and multiple lung nodules consistent with pulmonary sarcoidosis.")
Fig. 2:
30 year old, admitted with fatigue and weight loss.
Coronal and sagittal T1...
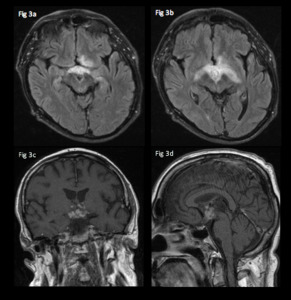
show expansion and vasogenic oedema affecting the optic chiasm and tracts bilaterally as a result of the hypothalamic inflammatory granuloma shown as multiple small enhancing and coalescing nodules on coronal (c) and sagittal (d) T1 post gadolinium.")
Fig. 3:
48 year-old male admitted with visual disturbance.
Axial FLAIR images...
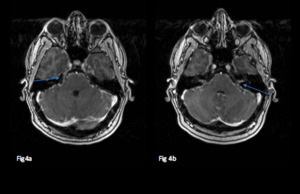
 and VII and VIII nerve complexes (b).")
Fig. 4:
50-year-old admitted with facial nerve deficits.
Axial T1 post gadolinium...

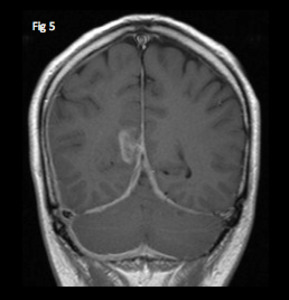
Fig. 5:
Coronal T1 with contrast shows diffuse thickening and enhancement of the falx...

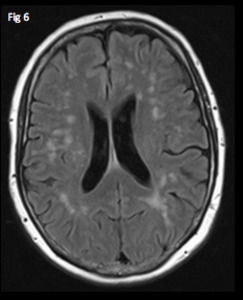
Fig. 6:
Axial FLAIR image at the level of the lateral ventricles shows multiple...
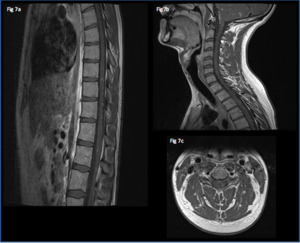
 and axial (c) T1 post gadolinium imaging shows peripheral intramedullary and leptomeningeal spinal cord involvement. Note also the posterior fossa leptomeningeal involvement on sagittal imaging of the cervical spine (b).")
Fig. 7:
27 year old, admitted with weight loss, headaches and ataxia.
Sagittal (a,b)...
 shows multiple tiny punctate hyperintensities within the lower cord, which enhance on T1 post gadolinium (b).
Axial FLAIR (c) in the same patient shows non-specific white matter hyperintensities.
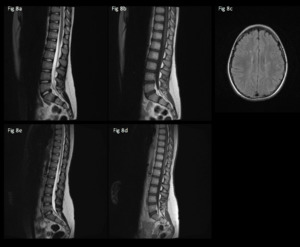
Sagittal T2 (e) and T1 post gadolinium (d) performed after treatment show complete resolution.")
Fig. 8:
12 year-old admitted with lower limb weakness, brisk reflexes and...