We performed retrospective review of imaging in obstructive jaundice patients presented to our Hospital through out-patiet department (OPD) clinic and emergency,
in a period of 3 years (from September 2014 to September 2017).
This descriptive observational study was approved from Hospital Ethic & Research Committee.
All adult patients (aged more than 15 years) for whom ultrasound,
CT scan and MRCP performed,
were included. Patients' ages range between 26 to 85 years. Only patients with extra-hepatic mechanical causes of biliary obstruction were included.
Paediatric patients (of less than 15 years) and those having intrahepatic mechanical or metabolic causes were excluded.
Patients who had already undergone intervention (biliary stenting) or surgery for primary liver,
gallbladder and panceatic tumors were excluded.
Patients for whom either CT or MRI study could not be performed (due to contrast-related issues,
claustrophia or other MRI contraindications) were also excluded.
Clinical data was obtained from HIS (Hospital Information System),
patients' files and charts.
Radiologic data was retrieved from RIS/ PACS (Radiology Information System/ Picture Archiving And Communication System).
Out of 225 patients,
only 75 patients were selected that were having all three radiologic imaging tests (ultrasound,
CT and MRCP) available on the system.
Transabdominal ultrasounds were performed using a curvilear probe.
Contrast enhanced porto-venous phase CT scans of abdomen were performed on a 128-slice CT scanner machine.
MRCP studies were performed on a 1.5-Tesla machine.
MRCP protocol included axial SSFSE (single-shot fast spin echo) BH (breath-hold) ARC (auto-calibrating reconstruction),
axial T2 RTr (respiratoy triggered) Propeller,
axial 2D FIESTA (fast imaging employing steady state acquisition) Fat sat,
Coronal SSFSE ARC,
Coronal T2 RTr Thin,
Coronal Cube T2 Navigation and Cor 3D MRCP RTr sequences.
Two radiologists having vast experience in body imaging (who were kept blinded of clinical information),
initially reviewed imaging findings independently (Cohen Kappa 0.62,
0.69 and 0.75; for ultrasound,
CT and MRCP respectively).
Mutually agreed findings were accepted in cases of minor discrepencies.
However,
in cases of major (diagnosis-related) discrepencies,
a consensus was developed amongst these two radiologists and a third senior one.
Imaging findings were documented as 'limited or non-diagnostic/ inconclusive/ equivocal',
and 'conclusive' (if a cause was ascertained) for all three modalities.
Final diagnosis was confirmed on ERCP findings and histopathology results (in cases of biopsies).
Individually,
ultrasound,
CT and MRCP could not detect cause of obstruction in 64% (n=48 patients),
36% (n=27) and 21% (n=16).
These were partly due to inherent limitations in these studies like obesity,
inadequate breath-hold (due to patient condition or age),
bowel gas obscuration in ultrasound,
less spatial resolution of CT (in detecting small lesions) and breathing artifacts related to MR imaging.
Ultrasound,
CT and MRCP were able to identify correct cause of obstruction in 24,
39 and 53 patients when compared with ERCP findings/ histopathologic results.
Diagnostic accuracies were measured separately [Table 2].
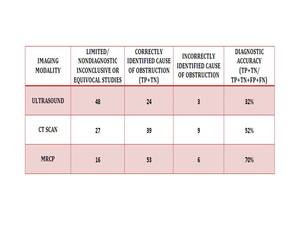
Fig. 4: Imaging modalities, results and their diagnostic accuracies
Table 2.
Imaging modalities,
results and their diagnostic accuracies
CT could detect correct cause or finding (TP & TN) in 39 patients (which included 12 patients of limited or non-diagnostic ultrasounds and 7 patients that were correctly diagnosed by ultrasound).
An 11 patients that were equivocal or inconclusive on CT were diagnosed correctly by ultrasound.
Therefore,
a sum of 50 patients were correctly diagnosed by combined ultrasound and CT.
Combined diagnostic accuracy of both ultrasound and CT was determined to be 66% whereas diagnostic accuracy of MRCP was found to be 70% (as 53 patients out of 75 were correctly diagnosed by this modality).
Ultrasound could easily detect biliary dilatation [Image 2],
stones as either casues of obstruction [Image 3] or of recenet stone passage when CBD was visulized clear till the pancreatic ampulla (and recent clinical history of biliary colic and known gallstones).
Choledocal cyst affecting proximal or mid segment CBD were also easily identifiable in patients with recurrent cholestasis.
Mirizzi's syndromes were also identified correctly by ultrasounds.
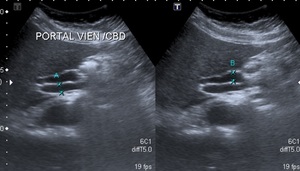
Fig. 5: Ultrasound showing dilated CBD
Image 2.
Spot split-screen ultrasound images showing dilated CBD
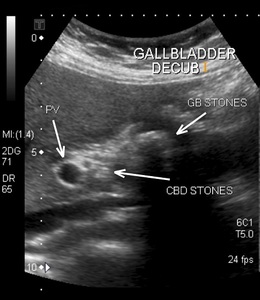
Fig. 6: Ultrasound showing stones within gallbladder and CBD
Image 3.
Spot ultrasound image showing gallbladder and CBD stones
CT could not detect tiny distal CBD stone (possibly due to their radiolucent characteristics and postion) or differentiate between sludge ball or debris at the distal end.
Surprisingly,
a couple of smaller ampullary lesions were picked up easily by CT [Image 4] than in MRCP (due to artifacts on MR imaging and unenhanced study).
CT could also detect correctly choledococeles and CA head of pancreas.
Concerns related to use of contrast (contrast allergies and renal impairment) and ionizing radiation were some important limitations in acquiring a CT examination in some patients.

Fig. 7: Sagittal reformat image of CT scan showing intra-luminal ampullary growth along distal CBD
Image 4.
Sagittal reformat contrast enhanced CT image showing subtly variable dense small ampullary lesion along distal CBD
MRI isolatedly was able to identify correct cause in majority of cases because of its intrinsic tissue contrast capabilities [Image 5 & 6].
Missed lesions were largely related to artifacts (due to inadequate breath-hold or movement) and possibly due to a non-contrast study.
An important implication of MRI was its exquisite ability to delineate biliary tree in 3D reformatted images that could detect variations in insertion of cystic duct (sometimes found low-lying) that were value for the surgeons particularly in subsequent laparoscpic cholecystectomy approach.
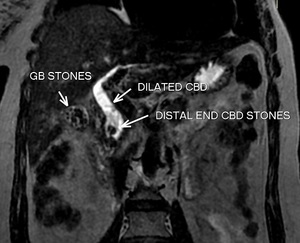
Fig. 8: Coronal Cube T2 reformat image showing obstructing stones in distal CBD
Image 5.
Coronal reformat thin T2W Cube image showing low intensity rounded stones obstructing the distal end of CBD
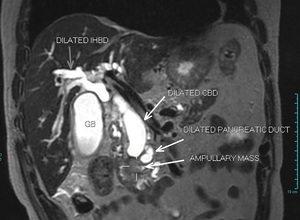
Fig. 9: Coronal Cube T2W reformat image showing ampullary mass obstructing the distal CBD and pancreatic duct
Image 6.
Coronal reformat image showing an ampullary mass obstructing both biliary and pancreatic ductal systems





