Disorders of the biliary tract affect a significant portion of the worldwide population,
and can pose problems in both diagnosis and management. Biliary obstruction refers to the blockage of any duct that carries bile from the liver to the gallbladder or from the gallbladder to the small intestine [Figure 1].
Cholestasis or failure of biliary flow may be due to biliary obstruction by mechanical means or by metabolic factors in the hepatic cells. Mechanical causes of biliary obstruction include intrahepatic and extrahepatic causes. Intracellular/ metabolic causes of cholestasis are very complex.
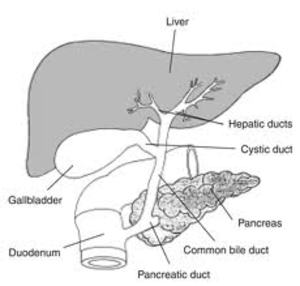
Fig. 2: Anatomy of Biliary tree
Figure 1.
Normal anatomy of biliary ductal system
Intrahepatic cholestasis generally occurs at the level of the hepatocyte or biliary canalicular membrane. Causes include hepatocellular disease (viral hepatitis,
drug-induced hepatitis),
drug-induced cholestasis, biliary cirrhosis, and alcoholic liver disease.
Extrahepatic obstruction to the flow of bile may occur within the ducts or secondary to external compression.
Overall, gallstones are the most common cause of biliary obstruction. Other causes of blockage within the ducts include malignancy, infection, and biliary cirrhosis. External compression of the ducts may occur secondary to inflammation (eg,
pancreatitis) and malignancy.
Regardless of the cause,
the physical obstruction causes a predominantly conjugated hyperbilirubinemia. Accumulation of bilirubin in the bloodstream and subsequent deposition in the skin causes jaundice (icterus) [Image 1].

Fig. 1: Icterus- a sign of jaundice
Image 1.
Icterus- a sign of jaundice
Conjunctival icterus is generally a more sensitive sign of hyperbilirubinemia than generalized jaundice.
Urine bilirubin is normally absent.
When it is present,
only conjugated bilirubin is passed into the urine as it is water soluble,
and may be evidenced by dark-colored urine [Table.
1]. The lack of bilirubin in the intestinal tract is responsible for the pale stools.
The cause of itching (pruritus) may be related to the accumulation of bile acids/bile salts in the skin.
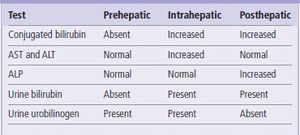
Fig. 3: Laboratory findings in Jaundice
Table 1.
Laboratory findings in Obstructive Jaundice
For patients in whom there is concern for obstructive jaundice,
the most commonly employed tests are ultrasound (US),
computed tomography (CT),
magnetic resonance imaging (MRI),
magnetic resonance cholangiopancreatography (MRCP),
and hepatobiliary 99mTc-iminodiacetic acid (HIDA) scans.
Other imaging modalities require more time,
sedation or specialist training.
They include endoscopic retrogradecholangiopancreatography (ERCP),
and percutaneous transhepatic cholangiography (PTC).


