ECR 2018 / C-0864
Correlation of findings on OGD and Contrast swallow.
Congress:
ECR 2018
Poster Number:
C-0864
Type:
Educational Exhibit
Keywords:
Swallowing disorders, Obstruction / Occlusion, Motility, Dynamic swallowing studies, Fluoroscopy, Gastrointestinal tract, Contrast agents, Stomach (incl. Oesophagus)
Authors:
L. Royle, S. Patel, N. Griffin; London/UK
DOI:
10.1594/ecr2018/C-0864

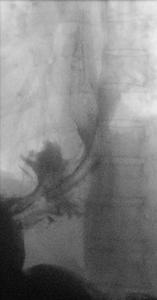
Fig. 1:
Lateral swallow demonstrating pharyngeal web where an OGD was normal.

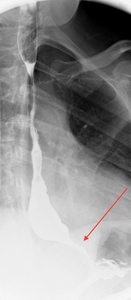
Fig. 7:
OGD was normal, swallow demonstrates tapering of the gastro-oesophageal...

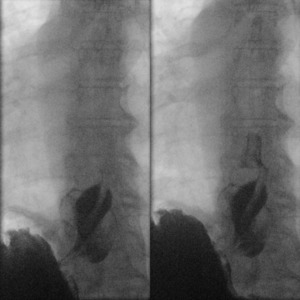
Fig. 8:
OGD demonstrated reflux oesophagitis, swallow study confirms the presence of...