Introduction
Obesity is an epidemic disease.
It is one of the main causes of preventable death.
In Mexico,
according to 2012 Encuesta Nacional de Salud y Nutrición (ENSANUT),
the prevalence of overweight and obesity in adults (Fig. 2) was 71.28% (representing 48.6 millon people).[1] Bariatric surgery is increasingly performed as a therapeutic alternative in obese patients who fail to lose weight with medical treatment.
The recommendations to perform a surgery include the following criteria: a BMI of 40 or higher,
or a BMI of 35 or higher in a patient with a high-risk condition such as severe sleep apnea,
obesity-related cardiomyopathy,
severe diabetes mellitus,
or failure of medical weight control.
Patients need a multidisciplinary approach including psychological evaluation to rule out psychiatric disorders or psychosocial factors that have been associated with a suboptimal surgical outcome. There are few contraindications to bariatric surgery including mental or cognitive impairment or severe coexisting medical conditions (coronary or liver disease).[2,3]
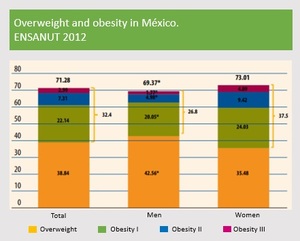
Fig. 2: Obesity prevalence in Mexico. The prevalence of obesity (BMI≥30 kg/m2) in adults was 32.4% and prevalence of overweight was 38.8%. Obesity was higher in the female sex (37.5%) than in the male (26.8%), in contrast to the overweight, where the male sex had a prevalence of 42.5% and the female sex of 35.9%. The combined prevalence of overweight and obesity is only 3.6 percentage points higher in the women (73.0%) than men (69.4%)
References: Encuesta Nacional de Salud y Nutrición. Ensanut 2012. Inst Nac Salud Pública. 2012:200. doi:10.1017/CBO9781107415324.004.
Bariatric surgical procedures reduce caloric intake by modifying the normal anatomy of the gastrointestinal tract,
and are classified as either restrictive which limit intake by reducing gastric capacity,
and malabsorptive which bypasses portions of small intestine where nutrients absorption occurs,
reducing the absorption surface,
other procedures combine both techniques (Fig. 3).
The laparoscopic Roux-en-Y gastric bypass has become the preferred method owing to decreased hospital stays and faster recovery and may be considered the standard of reference for bariatric surgery.
There are other procedures that are no longer performed due to low success rates and high incidence of complications such as jejunoileal bypass and biliopancreatic diversion or duodenal switch.[4]
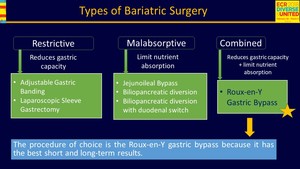
Fig. 3: Types of Bariatric Surgery
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX
Surgical technique[4-6]
The laparoscopic Roux-en-Y gastric bypass has evolved significantly since Wittgrove and Clark developed their technique in the early 1990s,
it is a combination of both mechanisms,
in which the gastric pouch serves as the restrictive component and the gastrojejunal anastomosis represents the malabsorptive component,
although the primary mechanism of weight loss is thought to be restrictive rather than malabsorptive.
Several variations are currently in use,
but in general involves stapling of the stomach to create a small (15-30 ml) upper gastric pouch with a larger excluded component (excluded stomach).
The small intestine is then divided at the midjejunum,
25-50 cm distal to the Treitz ligament,
and the distal portion (called the alimentary,
or Roux limb) is anastomosed to the gastric pouch by an end-to-end or an end-to-side anastomosis creating a blind ending jejunal stump.
The gastrojejunal anastomosis can be anterior or posterior to the transverse colon,
and is fashioned as a small caliber stoma (8-12 mm in diameter) to limit the emptying of solid food to the alimentary limb.
The proximal small intestine (the biliopancreatic limb) is anastomosed end-to-side 75-150 cm distal to the gastrojejunal anastomoses to the jejunum creating a common channel that continues to the ileum (Fig. 4).
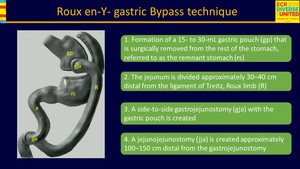
Fig. 4: Roux-en-Y gastric bypass surgical technique
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX

 in adults was 32.4% and prevalence of overweight was 38.8%. Obesity was higher in the female sex (37.5%) than in the male (26.8%), in contrast to the overweight, where the male sex had a prevalence of 42.5% and the female sex of 35.9%. The combined prevalence of overweight and obesity is only 3.6 percentage points higher in the women (73.0%) than men (69.4%) References: Encuesta Nacional de Salud y Nutrición. Ensanut 2012. Inst Nac Salud Pública. 2012:200. doi:10.1017/CBO9781107415324.004.")

