Postsurgical assessment and normal imaging findings
The knowledge of postoperative anatomy is crucial to rule out complications in the immediate and late postoperative period,
especially those that are life threatening.
Each surgical technique has its own special characteristics and the different types of complications must be recognized.[4]
Upper gastrointestinal examination is the modality of choice for immediate post-surgical evaluation of patients who have undergone this procedure,
it has a specificity close to 100%.[7,8] In our institution it is performed routinely to all patients in the first 24-48 post-surgical hours. The protocol consists of an initial scout film of the abdomen in upper position.
Then on the fluoroscopic table,
basically three positions are used with the patient standing,
left lateral oblique (Fig. 5a),
anterior-posterior (Fig. 5b),
and lateral (Fig. 6),
of these,
the first,
is the most useful since it reduces the superposition of structures.[6] Approximately 50 mL of a combination of water-soluble material is oral administered and if no leaks are found,
barium is given for the best characterization of the structures.
Fluoroscopy is performed as the patient swallows the contrast,
and images are obtained of the esophagus,
gastric pouch,
and jejunum.[7,8]
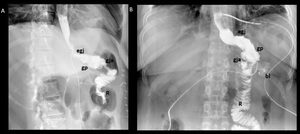
Fig. 5: Roux-en-Y gastric bypass normal post-surgical anatomy. Left lateral oblique (A) and anteroposterior (B) fluoroscopic spot image showing normal postoperative anatomy Roux-en-Y gastric bypass: esophagogastric junction (egj), gastric pouch (gp), Roux limb (R), blind ending jejunal stump (bl), result of the side-to side approach, and gastrojejunal anastomosis (gja).
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX
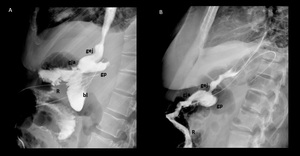
Fig. 6: Normal imaging findings after Roux-en-Y gastric bypass. A and B lateral fluoroscopic spot images showing opacified esophagogastric junction (egj), gastric pouch (gp), Roux limb (R), blind afferent limb (bl), and gastrojejunal anastomosis (gja).
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX
The imaging findings that we must identify are ( Fig. 7 ):[4,8]
- The gastric pouch,
which is identified immediately below the esophagus as a small structure,
with a volume of approximately 20 ml (15-30 ml).
- The gastrojejunal anastomosis,
which may be inferior,
posterior or anterior.
Under normal conditions the contrast material must pass freely through it to the Roux limb.
- The Roux limb,
which is a jejunum limb that should allow adequate passage of the contrast material and preserve its normal caliber.
- The study ends when the loop is opacified below the jejunum-jejunum anastomosis.
- Fifteen-minute delayed films are obtained to evaluate the pouch’s emptying capacity and to assess for leaks or reflux into the duodenum.
Fig. 7: Normal upper GI examination. The images show an adequate passage of water soluble contrast material from the esophagus (E) to the gastric pouch (gp) and then to the Roux limb (R) through the gastrojejunal anastomosis (gja).
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX
Roux-En-Y Gastric Bypass Complications
In the largest series,
the mortality rate associated with bariatric surgery is 0.1% to 2.0% (0.5% for gastric bypass,
0.1% for gastric banding,
and 1.1% for malabsorptive procedures).
Common causes of death among patients undergoing bariatric surgery include pulmonary embolism and anastomotic leaks.[4,7]
The complications are divided into early,
those that appear within the first post-surgical month,
and those that occur after this time are considered late (Fig. 8),
for its assessment,
several imaging methods are used,
the preferred method is the upper gastrointestinal series,
especially in the immediate post-surgical period.[8] After this time and depending on the clinical suspicion the evaluations can also be done with both oral an intravenous contrast abdominal CT.[6,9]
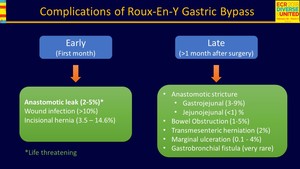
Fig. 8: Complications of Roux-en-Y Gastric Bypass
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX
It is the most feared early complication because it is life threatening due to the risk of abscess formation,
peritonitis,
and sepsis with a mortality rate higher than 5%. It is observed in up to 5% of patients and usually occurs within 10 days of surgery.
It most often occurs in the gastrojejunal anastomosis (65%),
although it is also seen at the gastric pouch,
jejunojejunostomy or blind ending jejunal stump.
Patients present with leukocytosis,
fever,
abdominal pain,
and tachycardia.
These clinical symptoms are non-specific,
and the clinical examination is limited by the patient habitus,
because of this,
the upper GI series are routine indicated 1 or 2 days after surgery.[4,10]
During the fluoroscopic study it is important to follow the contrast column through the gastrojejunal anastomosis before the intestinal loops with contrast overlap.
Leakage of contrast material can be identified directly,
observing the contrast extravasation (Fig. 9,
Fig. 13),
indirectly when an air-fluid level (Fig. 11) appears on the left upper quadrant (75% of the leaks extend to the left of the gastrojejunal anastomosis),
or when contrast material enters and passes through the drainage catheters.
[4,9]
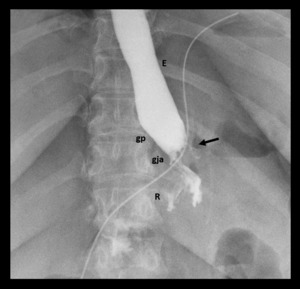
Fig. 9: Gastrojejunal anastomotic leak. Supine spot image from upper GI examination with water-soluble contrast material shows focal extravasation (black arrow) from left lateral aspect of gastrojejunal anastomosis (gja).
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX
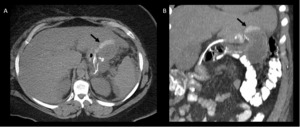
Fig. 10: Same patient from fig. 9, axial (A) and coronal (B) images of abdominal CT with oral contrast material show an extravasation (black arrows) of contrast material due to gastrojejunal anastomotic leak.
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX
Fig. 11: Roux-en-Y gastric bypass with postoperative anastomotic leak. Fluoroscopic images from an upper GI examination with water-soluble contrast material shows focal extravasation from left lateral aspect of gastrojejunal anastomosis into a large track and adjoining extraluminal collection.
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX

Fig. 12: Same patient of fig. 11, coronal image of abdomen CT with oral contrast, shows a collection with great air content in the upper left quadrant (c).
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX
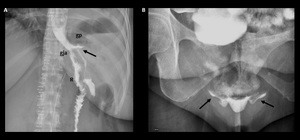
Fig. 13: Supine spot image from upper GI examination with water-soluble contrast material shows focal leak (arrow) from proximal stomach laterally into extraluminal collection in left upper quadrant (a). A delayed film shows free intraperitoneal contrast material.
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX
Staple line leaks are caused by staple line dehiscence which leads to a restored communication between the gastric pouch and the excluded stomach with subsequent fistula formation and has been reported in up to 3.5%.
It causes patient overeating,
less weight loss than expected,
or weigh gain.
At upper GI series and abdominal CT,
a fistulous tract arising from the pouch may opacify the excluded stomach (Fig. 14). It can be suspected on CT when contrast material is observed in the excluded stomach and in the absence of opacification of the biliopancreatic limb and duodenum.
All staple line leaks need a new intervention.[4,6]
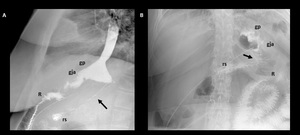
Fig. 14: Staple line dehiscence. Lateral (A) and anterio-posterior (B) fluoroscopic spot images show a fistulous tract (black arrows) between the gastric pouch (gp) and excluded stomach (rs) due to staple line dehiscence.
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX
- Anastomotic narrowing and strictures:
During the early post-operatory period it is normal to observe a transient narrowing of the anastomosis due to edema and spasm,
but passage of contrast material is ultimately allowed,and it usually resolves on the first days after the surgery ( Fig. 15a, Fig. 16 ).[4]
Strictures of the anastomosis are a long-term complication,
usually developing 4 weeks after surgery.
Factors that contribute to the development strictures include tension and ischemia at the anastomosis,
and the tissue restoration capacity of individual patients.
Patients present with symptoms derived from early satiety (progressive dysphagia,
vomiting,
abdominal pain,
and bloating).[11]
On upper GI series anastomotic strictures appear as short narrowed segments at the gastrojejunal anastomosis.
When there is an obstruction,
the gastric pouch is dilated,
and emptying of the contrast material towards the Roux limb is delayed (Fig. 15b,
Fig. 17).
The best projection to visualize strictures is the oblique because the localization of the anastomosis can be inferior,
anterior or posterior to the gastric pouch.[6,7] Most patients have an excellent response to endoscopic dilation; however,
some will require a new surgical intervention.[11]
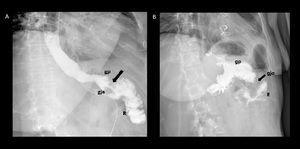
Fig. 15: Supine spot images from an upper GI examination with water- soluble contrast material. A) Postsurgical gastrojejunal anastomosis edema, a decrease in the caliber of the anastomosis (gja) is observed, but the contrast material passes form the gastric pouch (gp) to the Roux limb (R). B) Anastomosis stricture, the gastric pouch is dilated, little passage through the gastrojejunal anastomosis caused by marked narrowing.
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX
Fig. 16: Immediate ppostsurgical upper GI examination. Images show narrowing of the anastomosis due to edema and spasm, but passage of contrast material form gastric pouch (gp) to Roux limb (R) through gastrojejunal anastomosis (gja) is ultimately allowed.
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX
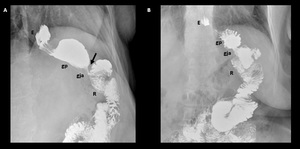
Fig. 17: Gastrojejunal anastomosis stricture in a patient who underwent to a Roux-En-Y Gastric Bypass 3 years ago. A) Oblique spot image showing a decreased caliber (black arrow) of the gastrojejunal anastomosis (gja) with dilation of gastric pouch (gp). B) Fifteen-minute delayed film shows an abnormal pouch´s capacity to emptying with retained contrast material.
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX
It occurs in up to 5% of patients.
It can be caused by adhesions,
internal hernias,
anastomosis strictures (Fig. 18) or intussusception.[4] The most common cause are internal hernias.
There are some factors that contribute to the development of internal hernias,
such as inadequate closure of mesenteric defects,
rapid excess weight loss following surgery leads to increased risk and may be more frequent when retrocolic technique is performed because three defects are created on the mesentery instead of two in anterocolic technique.
Incarceration of small bowel in an internal hernia can lead to obstruction,
infarction,
and perforation of strangulated loops.
Confirming the diagnosis of an internal hernia in a gastric bypass patient can be challenging.
Patients may report recurrent nonspecific,
colicky mid-epigastric or peri-umbilical pain.
The diagnostic requires knowledge of postoperative anatomy.
Imaging findings include clustered loops and migration of the anastomotic jejunojejunal suture line to the left midabdomen into the left upper quadrant.[9,11]
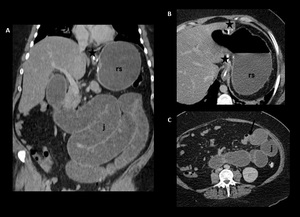
Fig. 18: Small bowel obstruction. Coronal (A) and axial (B, C) CT images after oral and intravenous contrast material administration show a collapsed gastric pouch (star), dilated excluded stomach (rs), and dilated small bowel loops (j). The transition zone is at the jejunaljejunum anastomosis (black arrow in C) which leads dilation of the biliary limb and excluded stomach.
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX
A marginal ulcer (stomal ulcer or anastomotic ulcer),
is defined as an ulcer that arises at or is near the gastrojejunostomy.
It is almost always located on the jejunal side of the anastomosis. They’ve been reported in 3-13% of patients and are thought to develop because of chronic exposure of the mucosa to acid entering the Roux limb.[4] Patients usually present with burning epigastric pain,
however,
it is not uncommon to find concomitant ulcers after other complications,
such as leaks,
internal hernia,
obstruction,
and even cholelithiasis.
Complicated or long-standing marginal ulcers may result in massive hematemesis or perforation of the gastrojejunostomy.
Some technical risk factors include a large gastric pouch,
use of nonabsorbable suture material,
and ischemia.
At upper GI series,
they are observed as ulcer niches at the gastrojejunal anastomosis or in the Roux limb.
Most marginal ulcer cases can be treated with proton pump inhibitors,
or sucralfate and conservative therapy.
In cases of complicated marginal ulcers surgical intervention may be needed.[7]
It is a very rare complication,
and it is reported sporadically and anecdotally.
It occurs due to recurrence of an anastomosis leak and the formation of a fistulous tract connecting the gastric pouch with the bronchial tree (Fig. 19).
Patients present with chronic cough,
sometimes associated with fluid or food intake,
hemoptysis,
and pleuritic pain.
The importance of a clinical suspicion,
is for deciding which type of contrast material to use,
since in these cases water-soluble material should not be given.[12]
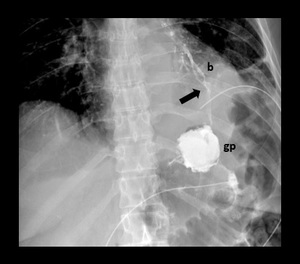
Fig. 19: Upper GI examination in a patient presenting chronic cough and repetitive pneumonia. Spot fluoroscopic image shows a fistulous tract (black arrow) connecting the gastric pouch (gp) with the bronchial tree (b).
References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX
There are other less common complications such jejunal ischemia caused by tension on the surgical mobilized jejunum,
intussusception which typically occurs at or near the jejunojejunal anastomosis,
and may be caused by the staple line acting as a leading point.
However,
the clinical suspicion is very important to get the right diagnosis.[7]

 and anteroposterior (B) fluoroscopic spot image showing normal postoperative anatomy Roux-en-Y gastric bypass: esophagogastric junction (egj), gastric pouch (gp), Roux limb (R), blind ending jejunal stump (bl), result of the side-to side approach, and gastrojejunal anastomosis (gja). References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX")
, gastric pouch (gp), Roux limb (R), blind afferent limb (bl), and gastrojejunal anastomosis (gja). References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX")
 to the gastric pouch (gp) and then to the Roux limb (R) through the gastrojejunal anastomosis (gja). References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX")

 from left lateral aspect of gastrojejunal anastomosis (gja). References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX")
 and coronal (B) images of abdominal CT with oral contrast material show an extravasation (black arrows) of contrast material due to gastrojejunal anastomotic leak. References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX")

. References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX")
 from proximal stomach laterally into extraluminal collection in left upper quadrant (a). A delayed film shows free intraperitoneal contrast material. References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX")
 and anterio-posterior (B) fluoroscopic spot images show a fistulous tract (black arrows) between the gastric pouch (gp) and excluded stomach (rs) due to staple line dehiscence. References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX")
 Postsurgical gastrojejunal anastomosis edema, a decrease in the caliber of the anastomosis (gja) is observed, but the contrast material passes form the gastric pouch (gp) to the Roux limb (R). B) Anastomosis stricture, the gastric pouch is dilated, little passage through the gastrojejunal anastomosis caused by marked narrowing. References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX")
 to Roux limb (R) through gastrojejunal anastomosis (gja) is ultimately allowed. References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX")
 Oblique spot image showing a decreased caliber (black arrow) of the gastrojejunal anastomosis (gja) with dilation of gastric pouch (gp). B) Fifteen-minute delayed film shows an abnormal pouch´s capacity to emptying with retained contrast material. References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX")
 and axial (B, C) CT images after oral and intravenous contrast material administration show a collapsed gastric pouch (star), dilated excluded stomach (rs), and dilated small bowel loops (j). The transition zone is at the jejunaljejunum anastomosis (black arrow in C) which leads dilation of the biliary limb and excluded stomach. References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX")
 connecting the gastric pouch (gp) with the bronchial tree (b). References: Radiology Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México/MX")