ECR 2018 / C-0936
Why Map the MAPCAs? : Heart to heart with a cardiac surgeon’
Congress:
ECR 2018
Poster Number:
C-0936
Type:
Educational Exhibit
Keywords:
Cardiac, Cardiovascular system, Paediatric, CT-Angiography, Image manipulation / Reconstruction, Computer Applications-3D, Education, Congenital, Developmental disease, Education and training
Authors:
P. Narang1, S. Arya2, A. K. Verma3, N. Goyal 4, D. S. Agarawal4; 1DELHI, DELHI/IN, 2Delhi/IN, 3New Delhi, Delhi/IN, 4New Delhi/IN
DOI:
10.1594/ecr2018/C-0936

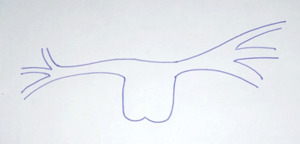
Fig. 3:
Pictorial depiction in patient with pulmonary atresia, showing confluent patent...

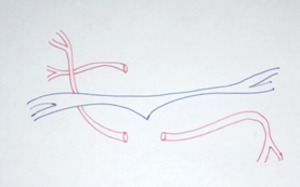
Fig. 4:
Pictoral depiction in patient with pulonary atresia, showing atretic pulmonary...

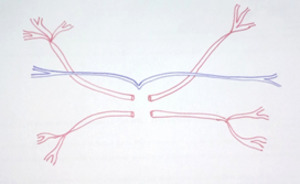
Fig. 5:
Pictorial depiction of process of Unifocalization

Fig. 6:
Axial maximum intensity projection image showing confluent pulmonary artery...

Fig. 7:
Axial images showing confluent pulmonary arteries with atretic main pulmonary...
 with VSD (red dotted line)")
Fig. 8:
Site of Stenosis: In patient with Infundibular stenosis (yellow arrow) with VSD...

Fig. 9:
Type A MAPCAS: Patient diagnosed with TOF with confluent pulmonary arteries...

Fig. 10:
TYPE B MAPCAS: Axial maximum intensity projection image showing atretic...
 on the right side. (b) showing the left pulmonary artery formed by a MAPCA from the descending thoracic aorta (yellow arrow).Note the arch on right side.(c) Right pulmonary
artery formed by a MAPCA from the descending thoracic aorta. (d) VRT image showing the reconstitution of the right pulmonary artery (yellow arrow) and the left pulmonary artery (red arrow) by the two MAPCAS from the descending thoracic aorta.")
Fig. 11:
TYPE C MAPCAS:Axial image showing VSD with the four cardiac chambers. Note the...
")
Fig. 12:
Axial images showing orign of MAPCAS from bilateral vertebral arteries (red...
 and right coronary RCA) arteries. MAPCAS can be seen arising from the LCX and the RCA (yellow and red arrows respectively).image")
Fig. 13:
Axial through the heart in a 2 year old male patient diagnosed as PS with...
")
Fig. 14:
Axial image showing MAPCAS from branches of aorta (red arrows)
")
Fig. 15:
MIP coronal, saggital and 3D volume rendered images showing MAPCAS arising from...
.")
Fig. 16:
MIP coronal, axial, 3D VRT and thick MIP coronal images showing MAPCAS arising...
 arising from left subclavian artery and descending thoracic aorta supplying right hilum.")
Fig. 17:
MIP axial and 3D VRT images showing MAPCAS (red arrow) arising from left...

Fig. 18:
In a patient of TOF, 3D VRT images and MIP saggital images showing priominent...
, hypoplastic right (RPA) and left pulmonary arteries(LPA). MAPCAs (yellow and orange arrows) arising from the descending aorta")
Fig. 19:
A 10 year old male patient of PA-VSD showing atresia of main pulmonary artery...
.")
Fig. 20:
Patient diagnosed as pulmonary atresia with VSD. Showing large MAPCAs supplying...
 and left hilum by small MAPCA (white arrow)")
Fig. 21:
Patient with complete atresia of MPA, RPA and LPA . Reconstitution of right...

Fig. 22:
Axial images showing MAPCAS of different sizes of MAPCAS.
 and encircling esophagus (white arrow).")
Fig. 23:
Axial images shows MAPCAS adjacent to trachea (green arrow in figure A) and ...

Fig. 24:
Patient with complete agenesis of pulmonary artery with VSD with different...

Fig. 25:
Dual supply to lungs from MAPACAS and pulmonary artery