Definition,
epidemiology and clinical features
DCIS is a breast malignancy that is characterized by the proliferation of malignant ductal epithelial cells,
without evidence of invasion of the basement membrane in microscopic evaluation (1).
Of all breast cancers detected at screening programs,
approximately 20%–25% are DCIS (1).
The importance of this pathology has increased due to a rise in the detection rate (secondary to the screening programs) and the controversy over its clinical significance,
required image diagnosis and treatment.
Early detection is of utmost importance as up to 40% of these lesions progress to invasive disease if they remain untreated.
The Van Nuys Prognostic Index,
which includes histologic grade,
is useful to decide which patients are at increased risk of progression andlocal recurrence,
thus allowing more accurate treatment decisions (11) (Table 1).
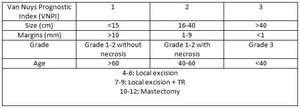
Table 1
There are no specific clinical manifestations for patients with DCIS.
Most patients will no present breast-related symptoms or findings on physical examination.
Before screening mammograms,
DCIS usually presented as a palpable mass,
nipple discharge,
or Paget's disease.
(2)
Imaging studies
Mammography
Mammography is the most important method for detecting DCIS.
Ninety percent of women with DCIS have suspicious microcalcifications on mammography and 75% of the time,
microcalcifications are the only finding of DCIS(6).
Less common findings include a mass,
soft tissue lesion (10%) or architectural distortion (7%–13%).
Including all findings,
the reported sensitivity of mammography for detection of DCIS is between 87% and 95% (3).
Some authors havedescribed a relation between mammography appearance and histologic grade.
Fine linear and fine linear branching morphologic features seen in a grouped or segmental distribution are usually associated with higher-grade DCIS,
whereas amorphous calcifications are associated with low-grade DCIS.
Low-grade DCIS has also been shown to appeared more frequently as a mass or asymmetry than high-grade DCIS.
(8,9) (Figure 1).
Ultrasonography (US)
When calcifications are identified at mammography,
US can evaluate anassociated mass component (infiltrative lesion) and allow US-guided biopsy,
less expensive and sometimes easier than aspiration biopsy. In that case,
specimen radiograph should be obtained to confirm the presence of calcification.
US appearance of DCIS depends on the presence of calcification.
Calcified DCIS most commonly manifests as echogenic foci located within a mass or a duct,
associated with microlobulations,
or distributed in branch pattern.
Noncalcified DCIS,
more often identified in symptomatic patients,
use to manifest as a hypoechoic mass with microlobulated margins and no posterior acoustic features (4) (Figure 2).
RM
MR imaging is more sensitive than mammography for determining the extent of disease.
DCIS may have variable morphologies on MR images,
with non-mass enhancement morphology as the most common manifestation.
Less commonly,
DCIS may also manifest as a mass on MR images,
in which case it is most likely to be irregular.
The kinetics of DCIS are also variable,
with fast uptake and a plateau curve reported as the most common kinetic pattern (6) (Figure 3).
The purpose of preoperative MR imaging is to determine tumor extension more accurately,
identify ipsilateral multicentric disease,
detect contralateral lesions and evaluate ganglionar affectation .
This information is very useful because the most important risk factors for DCIS recurrence are post-excision positive margins and synchronous foci that were not removed.
The findings in MR imagine can change the treatment of DCIS in some patients,
and its impantation in clinical practice could meanan improvement in patients assistance.
The purpose of our study is to quantify the number of cases in which performing a MR mean a change in treatment.
In previous revisions,
Liberman et al (5) reported that 5% of women who underwent bilateral breast MR imaging to determine disease extent were found to have mammographically occult malignancies in the contralateral breast,
half of which were DCIS.
Treatment
Patients with ductal carcinoma in situ (DCIS) are subsidiary of local treatment with mastectomy or breast-conserving therapy (BCT).
BCT consists of lumpectomy (also called wide excision,
or partial mastectomy) followed in most cases by adjuvant radiation.
Radiation therapy (RT) reduces the odds of breast recurrence but does not change the risk of distant recurrence or decrease mortality.
Radiation therapy may be reasonably omitted in a select population of patients withlow-risk disease (small foci of low-grade disease rejected with negative margins),
specially in case ofadvanced age,
extensive co-morbidities,
or patient preference.
Although mastectomy achieves excellent long-term survival with a low local recurrence rate,
it provides overly aggressive treatment for many women.
BCT has less morbidity but is associated with a higher risk of local recurrence.
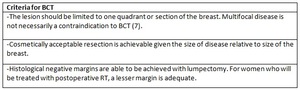
Table 2



 that were not present in previous studies (left image). Biopsy specimens showed high-grade DCIS.")

 morphology is the most common manifestation. In images above, we can see an intermediate-grade DCIS in a 45-year-old woman ; a) T2 fat supression, b) T1 thrive postcontrast, c) dynamic contrast enhance and d) digital subtraction")