The wide spectrum of acute biliary disorders is established as a result of different pathological conditions: inflammatory/infectious conditions,
obstructions,
perforations and trauma.
We describe the biliary emergency conditions in which the MRI could provide more information than CT and US.
Inflammatory/infectious diseases
Acute cholecystitis is a very common surgical emergency.
In about 90%-95% of cases,
acute cholecystitis is caused by gallstone impaction in the neck of the gallbladder or cystic duct.
As a result of the obstruction,
bile stasis,
ischemia,
and development of systemic infection can occur.
US and CT are the investigations of choice and in most cases they allow a correct diagnosis both in simple acute cholecystitis and in most common complications of acute cholecystitis.
MRCP, and in selected cases the contrast-enhanced MR imaging (ce- MRCP),
with intravenous injection of hepatospecific contrast-media may be useful in risk stratification of the patients with acute cholecystitis.
It is known the relationship between cystic duct patency and the severity and course of the disease.
Totally obstructed duct may provide a progressive disease course and predispose to a higher chance of developing complications,
while a substantial patency of the duct may suggest simple acute cholecystitis or chronic cholecystitis. In asymptomatic fasting patients,
in the absence of liver dysfunction,
the gallbladder typically fills (using Gd- EOB-DTPA) within 15-20 min after injection and fills within 30 min in 95% of cases.
Delayed filling or lack of filling of the gallbladder on MRCP support confirmation of diagnoses of acute cholecystitis Fig. 1
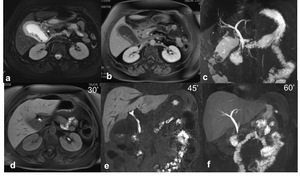
Fig. 1: Acute cholecystitis. (a) Axial TSE T2 fat sat (b) axial contrast e-enhanced SPGR 3D T1, (c) MRCP single-shot TSE T2 MIP(d-e-f) axial and coronal contrast enhanced SPGR 3D hepatobiliary phase at 30, 45 and 60 minutes’ show presence of gallstone, diffuse thickening of the gallbladder walls with high signal in T2W. After 60 minutes from administration of Gb-EOB was proved the absence of patency of the cystic duct, so confirming the diagnosis of acute cholecystitis
References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
Ascending cholangitis is a condition determined by an impacted stone in the common bile duct which causes biliary stasis and infections (80%),
while only 20% obstructions is due to malignant causes.
The diagnosis is based on clinical and laboratory data,
but the imaging has the task of identifying the site of the obstruction and characterize the cause.
In this conditions MR may provide more data than CT and the US.
MRI accuracy is about 94% and shows:
- dilation of the biliary tract;
- thickening of the wall of the bile ducts;
- transient hepatic intensity difference (THID) secondary to periductal hyperaemia phlogosis or decreased portal perfusion;
- parenchymal abscesses.
Contrast-enhanced MR images help in differentiating other pathologies,
such as rupture of cysts from echinococcosis in communication with the biliary duct,
biliary candidiasis or neoplastic processes,
that can be recognized as ascending cholangitis due to lithiasis.
Fig. 2
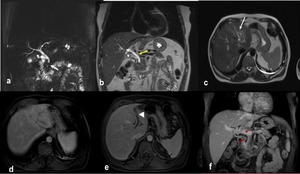
Fig. 2: Ascending cholangitis. (a) MRCP MIP 3d T2, (b-c) coronal and axial single-shot TSE T2 show mildly dilatation of the intra and extrahepatic bile duct (white and yellow arrows, b-c), due to lithiasis of the distal common bile duct (white arrows, a). Axial and coronal contrast-enhanced SPGR 2D T1 (d-e-f) show in the arterial phase (d) transient hyperemia (THID) of the second, third and fourth hepatic segment due to thrombosis of the left portal branch (arrowhead, e) and bright enhancement of the common bile duct and intra-hepatic biliary duct walls (red arrows, f).
References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
Obstructions
It can be caused by stones or benign and malignant strictures.
Mirizzi syndrome or cholecisto-choledocic fistula is the result of the gallstone passage in the neck of the gallbladder or in the cystic duct; the compression exerted on the common hepatic duct determines the gradual erosion of the common hepatic duct wall and the formation of a cholecysto-choledocic fistula related to recurrent episodes of cholangitis.
MRI improves diagnostic accuracy,
more than other imaging techniques and allows the assessment of the:
- dilatation of intrahepatic biliary duct;
- site of obstruction;
- narrowing of the common hepatic duct caused by impacted gallstone in the gallbladder neck,
cystic duct or in the common bile duct.
Fig. 3
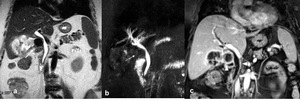
Fig. 3: Mirizzi syndrome, type I. (a) Coronal single-shot TSE T2, (b)MRCP MIP TSE T2 and (c) coronal contrast-enhanced SPGR 2D T1 show external compression of the main bile duct by a gallstone wedged in the infundibulum of the gallbladder (arrows), which appears distended and with inhomogeneous content. After contrast-medium injection an intense enhancement of the gallbladder wall and biliary duct (arrowheads) is shown.
References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
Fig. 4
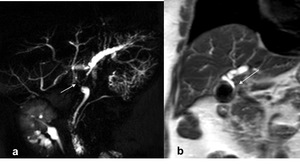
Fig. 4: Mirizzi syndrome, type II. (a) MRCP MIP 3D T2 and (b) coronal single-shot TSE T2 show the presence of gallstone which impacted in the cystic duct (arrows) causing external compression of the main bile duct with mild dilatation of the intrahepatic biliary tree.
References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
Fig. 5
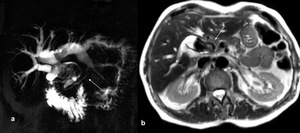
Fig. 5: Mirizzi syndrome, type III. (a) MRCP single-shot TSE T2 single-slab and (b) axial single-shot TSE T2 show diffuse dilation of the intrahepatic bile ducts associated with anatomical variant for independent confluence of the postero-lateral bile duct into the common bile duct, which appears dilated and almost completely occupied by massive gallstone (arrows).
References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
Fig. 6
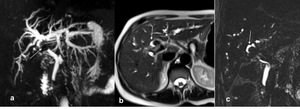
Fig. 6: Mirizzi syndrome, type IV. (a) MRCP MIP TSE T2, (b) axial single-shot TSE T2 and (c) MRCP TSE T2 3D show diffuse dilatation of intrahepatic bile duct due to massive obstructing gallstone in the confluence of the hepatic duct (arrow, a) with a collapsed gallbladder (arrow, b and c).
References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
Fig. 7
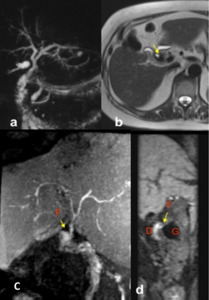
Fig. 7: Mirizzi syndrome, type IV with Choledocho-duodenal fistula. (a) MRCP single-shot TSE T2 MIP and (b) axial single-shot TSE T2 show gallstone in the bile duct without dilatation of biliary tree and small hyperintensity next to the common bile duct (yellow arrow, b). (c) coronal contrastenhanced SPGR 3D T1 MIP and (d) reformatted in sagittal plane in hepatobiliary phase reveal the presence of a fistula between the common bile duct and duodenum. [legenda: gallstone (G), duodenum (D) and site of fistula (F)].
References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
Strictures
Benign and Malignant biliary obstruction (Tab.1) does not occur acutely in the same manner as choledocholithiasis,
but patients may present in emergency with obstructive jaundice and complicating cholangitis as the growing tumour occludes the biliary tree.
Cholangiocarcinoma Fig. 8,
gallbladder carcinoma,
ampullary tumours,
and pancreatic adenocarcinoma may result in an obstruction of the biliary tree once they have progressed.
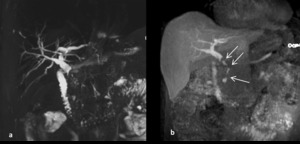
Fig. 8: Biliary stricture in patient with intraductal cholangiocarcinoma: the cholangiographic-image MIP 3D T2 (a) shows the biliary dilatation secondary to an apparent long and tight stenosis of the middle-distal common bile duct; the image MIP excretory (b) indicates multiple intraluminal filling defects (arrow) with partial stenosis and preserved excretion of the contrast agent in duodenum.
References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
Benign strictures are extremely rare and are located in the hepatic hilum or at the distal VBP.
Clinically,
benign biliary strictures can present with a wide array of manifestations ranging from being completely asymtomatic to showing overt clnical and laboratory evidence of biliary obstruction.
The causes of benign stenosis are multiple .
Tab.1
|
Malignant and benign bile duct strictures
|
|
Malignant strictures
|
|
Cholangiocarcinoma
|
|
HCC
|
|
Carcinoma of the gallbladder
|
|
Ampullary carcinoma
|
|
Lymphoma of the VB
|
|
Intrabiliary metastasis
|
|
Melanoma of the VB
|
|
Leukemic involvement of the biliary system
|
|
Carcinoid of the bile ducts
|
|
Benign strictures
|
|
Primary sclerosing cholangitis
|
|
IgG4-related disease
|
|
Mirizzi syndrome
|
|
Recurrent pyogenic cholangitis
|
|
HIV cholangiopathy
|
|
Sclerosing cholangitis induced by chemotherapy
|
|
Iatrogenic stenosis
|
|
Anastomotic and non-anastomotic
|
|
Chronic pancreatitis
|
|
Portal Biliopathy
|
|
Oddi dysfunction
|
|
Miscellaneous: TB,
sarcoidosis,
cystic fibrosis
|
MRI permits to characterize the benign (Fig.
9) or malignant strictures and identify the level of obstruction choosing the right therapy like: percutaneous biliary decompression,
endoscopic stent placement,
or surgical resection.

Fig. 9: (a) MRCP MIP TSE T2. (b) coronal MIP SPGR 3D T1 in hepatobiliary phase. (c-d) Coronal and axial SPGR T1 in hepatobiliary phase. Combined performance of T2W and T1 post-contrast MRCP in patient with IgG4 related cholangiopathy provide comprensive images work up including morphological and functional information with better graduation of biliary stenosis (arrow) and liver parenchimal enhancement (*)
References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
Perforations
Gallbladder perforation: is a life-threatening complication of acute cholecystitis occurring in approximatively 2-11% of patient and needs surgery.
The most frequent site of perforation is the fundus as it collects less amount of blood supply.
Niemeier,
in 1934,
suggested a classification of gallbladder perforation.
- Type I: acute free perforation of the gallbladder into the peritoneal cavity (16%) is burdened by high mortality.
MRI findings are:
- disruption of the gallbladder wall,
TSE T2W half-Fourier sequences are particularly useful to demonstrate discontinuity of the gallbladder wall;
- Ce-MRCP may identify the wall defects and shows leaks of contrast medium into the peritoneal cavity during excretory phase;
- gallbladder lumen collapsed or not displayed;
- pericholecystic fluid;
- extra luminal gallstones;
- thick peritoneum,
with or without ascites.
Fig. 10
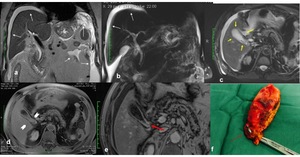
Fig. 10: Gallbladder perforation, Type I. (a) Coronal single shot TSE T2, (b) MRCP MIP 3D T2, (c) Axial T2-W SPAIR and (d-e) contrast-enhanced SPGR 2d T1 show ascites and thick peritoneum (white arrows, a and b) , diffuse and irregular mural thickening of gallbladder wall and pericholecystic fluid (yellow arrows, c) with gallbladder mild distended (arrowhead2) and on contrast-enhanced imaging show a tiny wall discontinuity charged to Hartmann's pouch (red arrow, e) which was found to be a small hole at surgery.
References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
- Type II: subacute perforation surrounded by a pericholecystic abscess walled off by adhesions (68%).
MRI shows:
- Presence of pericholecystic abscess (intrahepatic or extrahepatic) with rim enhancement in contrast-enhanced T1W imaging;
- Ce-MRCP may show filling of the gallbladder with concurrent filling of pericholecystic abscess thus proving a communication. Fig. 11
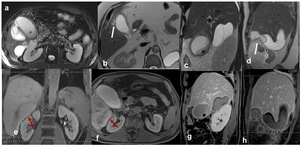
Fig. 11: Gallbladder perforation, Type II. (a) Axial TSE T2 fat sat (b-c-d) axial and sagittal single-shot TSE T2 show disruption of the gallbladder wall (arrows) and communication between gallbladder lumen and intrahepatic fluid collection and display a perihepatic fluid collection (c and d). The study carried out in the hepatobiliary phase (e-f-g-h) axial and sagittal contrast-enhanced SPGR 3D T1 demonstrates also the passage of the contrast-media in the perihepatic fluid collection (red arrows, e and f)
References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
- Type III: chronic perforation with presence of a fistulous communication between gallbladder and bowels (16%).
Cholecysto-duodenal is the most common form and occurs in 70% of cases Fig. 12; cholecisto-colic occurs in 14% of cases and cholecisto-gastric in 6%.
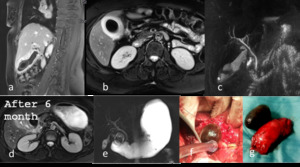
Fig. 12: Cholecysto-duodenal fistula.
First hospital admission: (a-b) Sagittal and axial TSE T2 fat sat (c) MRCP MIP T2 showed gallbladder over distended with intraluminal gallstone, thickened gallbladder wall with hyperintensity on T2 fat-sat images of the pericholecystic tissue.
After 6 months, MRI (d) TSE T2 fat sat and (e) MRCP Single-Shot T2 2D showed not lying gallbladder with extra luminal gallstone migrated into duodenum, resulting in a significant duodenal stenosis with associated gastric dilatation. Finding confirmed by surgery (f-g).
References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
MRI findings of this condition are:
- pneumobilia in absence of anamnestic data of previous surgical or endoscopic procedures;
- collapsed aspect of the gallbladder;
- ectopic stones sometimes responsible for obstructive digestive syndrome (gallestones ileus,
Bouveret Sindrome) Fig. 13
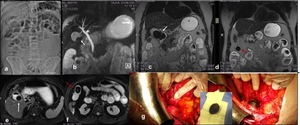
Fig. 13: Biliary ileus. (a) Abdominal X-ray (b) MRCP MIP 3D T2, (c-d) coronal single-Shot T2 2D(e-f) axial TSE T2 fat-sat show air-fluid level (a) with over-distension of the bowel loops (b); massive gallstone in the gallbladder (c and e) with bilio-digestive fistula (c) there is also another ectopic gallstone (red arrow, d and f) resulting in jejunal obstruction. The patient was treated surgically (g) and these findings were confirmed.
References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
Trauma
Causes of biliary trauma
- Blunt abdominal trauma (motor vehicle deceleration injuries,
falls,
assaults) or penetrating injury caused by a simple direct force (knife wound) or by a complex,
indirect injury (gunshot wound).
Fewer than 40 cases of common bile duct avulsion following are reported; however,
blunt trauma is much more rare than penetrating trauma and more difficult to diagnose. Occurs in 2% of blunt trauma victims.
The low incidence is attributed to the organ’s well-protected location.
They are associated with others intraabdominal injuries (Liver injury : 83–91%.
Duodenum and spleen injuries: 54%).
It is a very rare condition,
with an high mortality related to vascular damage of the hepatoduodenal ligament.
There is no standard approach to the early diagnosis of these injuries.
Imaging findings are:
- Active extravasation of bile;
- Focal perihepatic or intrahepatic fluid collections;
- Ascites;
- Liver lacerations
Contrast-enhanced computed tomography and US are the conventional initial studies,
which allow definition of the site,
identification,
and eventually,
draining of fluid collections,
but they provide limited information about associated biliary tree lesions.
A comprehensive MR examination that includes both MRCP and Ce-MRCP should be recommended in patients with suspicion gallbladder-biliary ducts injuries in order to characterize the fluid with direct view of the progressive enhancement during the excretory phase and identificate more accurately the anatomic site of rupture (Fig. 14).
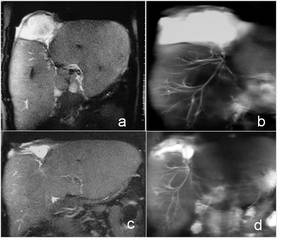
Fig. 14: 14 years old boy. Large laceration of the IV segment of the liver after a car accident, documented on a T2 coronal image (a). The MRCP control shows a lesion of a segmental branch that feeds the collection(b).Next control after cutaneous drainage placement demonstrates a significant reduction of the collection in the coronal T2 and MRCP images.
References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)"
2.
Iatrogenic bile duct injury during laparoscopic cholecystectomy:
is a rare cause of acute biliary obstruction,
it may occur during liver transplant,
hepatic resection,
or cholecystectomy.
The rate of iatrogenic bile duct injury is low,
with reported rates of 1.0% for laparoscopic and 0.5% for open cholecystectomy.
Causes :
- Direct trauma by grasping forceps;
- Excessive dissection around the porta hepatis with tearing of the common bile duct wall;
- Improper placement of clips lacerating the EBT;
- Iatrogenic stenosis (direct complication of the T-shaped drainage tube or as a result of thermic damage)
It is related with substantial need for a new intervention,
increased hospital costs,
and decreased quality of life for the patients.
MRCP in an ideal diagnostic test whenever bile duct injury following L.C.
is suspected. MRCP can accurately diagnose postoperative strictures and excision iniuries and can characterize and anatomically classify these injuries for planning preoparative surgery.
The combined use of T2 MRCP and Ce-MRCP has been very effective in recognizing the level of iatrogenic stenosis compared to the only T2 MRCP with a favourable impact on the choice of the therapeutic option ( Fig.
15 )
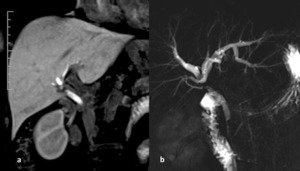
Fig. 15: Iatrogenic stenosis. Cholangiographic T2 2D image (a) shows a iatrogenic stenosis that involves the common bile duct (CBD) at < 2 cm from the carrefour without involvement of the posterior right biliary duct that has an aberrant drainage in the CBD, resulting in fact not dilated. The Ce-MRCP MIP 3D T1 image (b) confirms the site of the stricture ( Bismuth II lesion) and shows a regular passage of the contrast medium downstream
References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)"
Gadolinium-based hepatobiliary contrast agents,
such as gadoxetate disodium,
play an important role in MRI.
The Contrast enhanced - MRCP allows to characterize the fluid with direct view of the progressive enhancement during the excretory phase and can highlight anatomic site of rupture,
damaged duct and high or low flow rate of the leak with an effect on the management of the patient.
(Fig.
16 )
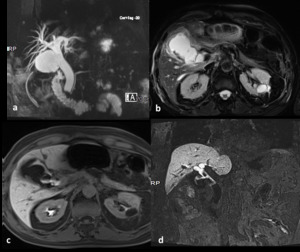
Fig. 16: Biloma secondary to a biliary leak five days after a cholecystectomy: The MIP 3D T2 (a) and axial T2 (b) images show the presence of a fluid collection; in the excretory study after Gd-BOPTA shows the progressive filling of a biloma(c-d) and indicates the site of damaged duct.
References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)"
Furthemore ,MR Angiography can be performed allowing the simultaneous evaluation of the biliary tree and hepatic vascular supply that is essential in case of concomitant bilio-vascular lesion.( Fig.
17)
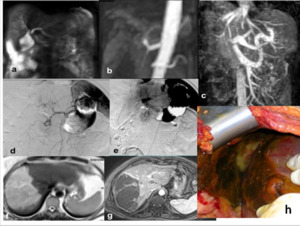
Fig. 17: Biliary and vascular iatrogenic lesions after laparoscopic cholecystectomy.
Iatrogenic lesion type IV according to Bismuth classification, with bile collection close to biliary carrefour (a).
The coronal angiographic MIP image in the arterial phase (b) demonstrates no visualization of the right branch of the hepatic artery with small ferromagnetic artefacts.
In portal phase (c), lack of representation of the right portal branch. These findings are confirmed by the angiographic examination (d-e) which also shows the presence of surgical clips close to common hepatic artery. The T2W FSE and T1 GE axial images after mdc (f-g) demonstrate an extensive area of the right hepatic lobe infarct, as confirmed by the intraoperative image (h).
References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)"

 Axial TSE T2 fat sat (b) axial contrast e-enhanced SPGR 3D T1, (c) MRCP single-shot TSE T2 MIP(d-e-f) axial and coronal contrast enhanced SPGR 3D hepatobiliary phase at 30, 45 and 60 minutes’ show presence of gallstone, diffuse thickening of the gallbladder walls with high signal in T2W. After 60 minutes from administration of Gb-EOB was proved the absence of patency of the cystic duct, so confirming the diagnosis of acute cholecystitis References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)")
 MRCP MIP 3d T2, (b-c) coronal and axial single-shot TSE T2 show mildly dilatation of the intra and extrahepatic bile duct (white and yellow arrows, b-c), due to lithiasis of the distal common bile duct (white arrows, a). Axial and coronal contrast-enhanced SPGR 2D T1 (d-e-f) show in the arterial phase (d) transient hyperemia (THID) of the second, third and fourth hepatic segment due to thrombosis of the left portal branch (arrowhead, e) and bright enhancement of the common bile duct and intra-hepatic biliary duct walls (red arrows, f). References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)")
 Coronal single-shot TSE T2, (b)MRCP MIP TSE T2 and (c) coronal contrast-enhanced SPGR 2D T1 show external compression of the main bile duct by a gallstone wedged in the infundibulum of the gallbladder (arrows), which appears distended and with inhomogeneous content. After contrast-medium injection an intense enhancement of the gallbladder wall and biliary duct (arrowheads) is shown. References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)")
 MRCP MIP 3D T2 and (b) coronal single-shot TSE T2 show the presence of gallstone which impacted in the cystic duct (arrows) causing external compression of the main bile duct with mild dilatation of the intrahepatic biliary tree. References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)")
 MRCP single-shot TSE T2 single-slab and (b) axial single-shot TSE T2 show diffuse dilation of the intrahepatic bile ducts associated with anatomical variant for independent confluence of the postero-lateral bile duct into the common bile duct, which appears dilated and almost completely occupied by massive gallstone (arrows). References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)")
 MRCP MIP TSE T2, (b) axial single-shot TSE T2 and (c) MRCP TSE T2 3D show diffuse dilatation of intrahepatic bile duct due to massive obstructing gallstone in the confluence of the hepatic duct (arrow, a) with a collapsed gallbladder (arrow, b and c). References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)")
 MRCP single-shot TSE T2 MIP and (b) axial single-shot TSE T2 show gallstone in the bile duct without dilatation of biliary tree and small hyperintensity next to the common bile duct (yellow arrow, b). (c) coronal contrastenhanced SPGR 3D T1 MIP and (d) reformatted in sagittal plane in hepatobiliary phase reveal the presence of a fistula between the common bile duct and duodenum. [legenda: gallstone (G), duodenum (D) and site of fistula (F)]. References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)")
 shows the biliary dilatation secondary to an apparent long and tight stenosis of the middle-distal common bile duct; the image MIP excretory (b) indicates multiple intraluminal filling defects (arrow) with partial stenosis and preserved excretion of the contrast agent in duodenum. References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)")
 MRCP MIP TSE T2. (b) coronal MIP SPGR 3D T1 in hepatobiliary phase. (c-d) Coronal and axial SPGR T1 in hepatobiliary phase. Combined performance of T2W and T1 post-contrast MRCP in patient with IgG4 related cholangiopathy provide comprensive images work up including morphological and functional information with better graduation of biliary stenosis (arrow) and liver parenchimal enhancement (*) References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)")
 Coronal single shot TSE T2, (b) MRCP MIP 3D T2, (c) Axial T2-W SPAIR and (d-e) contrast-enhanced SPGR 2d T1 show ascites and thick peritoneum (white arrows, a and b) , diffuse and irregular mural thickening of gallbladder wall and pericholecystic fluid (yellow arrows, c) with gallbladder mild distended (arrowhead2) and on contrast-enhanced imaging show a tiny wall discontinuity charged to Hartmann's pouch (red arrow, e) which was found to be a small hole at surgery. References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)")
 Axial TSE T2 fat sat (b-c-d) axial and sagittal single-shot TSE T2 show disruption of the gallbladder wall (arrows) and communication between gallbladder lumen and intrahepatic fluid collection and display a perihepatic fluid collection (c and d). The study carried out in the hepatobiliary phase (e-f-g-h) axial and sagittal contrast-enhanced SPGR 3D T1 demonstrates also the passage of the contrast-media in the perihepatic fluid collection (red arrows, e and f) References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)")
 Sagittal and axial TSE T2 fat sat (c) MRCP MIP T2 showed gallbladder over distended with intraluminal gallstone, thickened gallbladder wall with hyperintensity on T2 fat-sat images of the pericholecystic tissue.
After 6 months, MRI (d) TSE T2 fat sat and (e) MRCP Single-Shot T2 2D showed not lying gallbladder with extra luminal gallstone migrated into duodenum, resulting in a significant duodenal stenosis with associated gastric dilatation. Finding confirmed by surgery (f-g). References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)")
 Abdominal X-ray (b) MRCP MIP 3D T2, (c-d) coronal single-Shot T2 2D(e-f) axial TSE T2 fat-sat show air-fluid level (a) with over-distension of the bowel loops (b); massive gallstone in the gallbladder (c and e) with bilio-digestive fistula (c) there is also another ectopic gallstone (red arrow, d and f) resulting in jejunal obstruction. The patient was treated surgically (g) and these findings were confirmed. References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)")
. The MRCP control shows a lesion of a segmental branch that feeds the collection(b).Next control after cutaneous drainage placement demonstrates a significant reduction of the collection in the coronal T2 and MRCP images. References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)"")
 shows a iatrogenic stenosis that involves the common bile duct (CBD) at < 2 cm from the carrefour without involvement of the posterior right biliary duct that has an aberrant drainage in the CBD, resulting in fact not dilated. The Ce-MRCP MIP 3D T1 image (b) confirms the site of the stricture ( Bismuth II lesion) and shows a regular passage of the contrast medium downstream References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)"")
 and axial T2 (b) images show the presence of a fluid collection; in the excretory study after Gd-BOPTA shows the progressive filling of a biloma(c-d) and indicates the site of damaged duct. References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)"")
.
The coronal angiographic MIP image in the arterial phase (b) demonstrates no visualization of the right branch of the hepatic artery with small ferromagnetic artefacts.
In portal phase (c), lack of representation of the right portal branch. These findings are confirmed by the angiographic examination (d-e) which also shows the presence of surgical clips close to common hepatic artery. The T2W FSE and T1 GE axial images after mdc (f-g) demonstrate an extensive area of the right hepatic lobe infarct, as confirmed by the intraoperative image (h). References: Departement of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)"")