We present:
A.
Breast lesions arising in different breast gland components:
1.Skin.
-Sebaceous cysts.
Epidermal inclusion cysts
They are the most frequent skin lesions,
caused by a proliferation of squamous epithelium within the dermis or epidermis.
Imaging findings ( Fig. 1 ).
• Mammograms. Usually circumscribed nodules .
• US.
Circumscribed hypoechoic or heterogeneous lesions with through transmission included in the dermal plane.
Inflammatory or ruptured lesions may present with ill-defined margins .
• MR.
Usually not studied with MR may appear as incidental findings.
Circumscribed lesions low-intermediate T1,
high T2.
On T1 with Gadolinium injection,
no contrast enhancement appears centrally but a thin peripheral enhancement may be depicted.
Ruptured cysts may show irregular rim enhancement and sometimes enhancement of adjacent tissues.
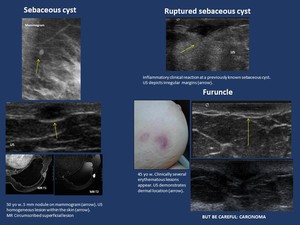
Fig. 1: Skin lesions
Differential diagnosis.
Clues.
Skin lesions are sometimes difficult to distinguish from those arising in the superficial area of the breast which moreover may also involve the overlying skin.
Radiologic features of the lesion should be carefully analysed to determine lesion location in order to make the correct differential diagnosis.
Most tumors involving only the dermal plane are benign,
but breast lesions which involve the skin are frequently malignant.
US is a helpful tool in differential diagnosis of superficial lesions ( Fig. 2 ). Mammogram cannot easily distinguish between skin and breast lesions.
MR depicts lesion location,
but due to its availability is not so accessible.
On US Dermal lesions appear either within the hyperechoic superficial layer or within the hypoechoic layer (subdermal fat) with a tract to surface.
Dermal lesion partially included in the breast plane present with dermal tissue surrounding them and an acute or 90º angle with the dermis,
whereas breast lesions invading the dermal plane appear with an obtuse angle with the dermis.
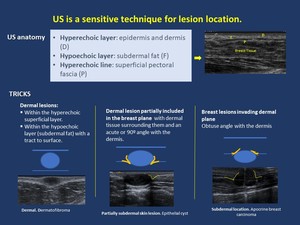
Fig. 2: Skin Imaging: Tips for US in lesion location.
2. Stroma
Two types of stroma are present in the mammary gland,
breast specific and non-specific stroma,
with different features:
-Breast specific or specialized stroma.
Mainly intralobular,
it covers the terminal duct-lobular unit (TDLU).
Loose,
myxomatous,
hormonally responsive stroma containing scattered lymphocytes and enclosing lobules.
-Non- specific stroma.
Usually interlobular,
it is a fibroconnective tissue,
causing breast lesions similar to those seen elsewhere in the body.
PATHOLOGY.
2.1.
Breast specific or specialized stroma.
2.1.1.Pseudoangiomatous stromal hyperplasia (PASH).
It is a benign stromal localized mesenchymal stromal cell overgrowth which is found most frequently in premenopausal women and clinically painless.
Usually it appears as an incidental finding,
a microscopic focus,
but may also show mass appearance on histopathology simulating a fibroepithelial tumor.
Moreover presentation may be solitary,
multifocal nodules or a diffuse massive process with asymmetry of the breast.
On immunohistochemistry it is positive for CD34 and progesterone receptors,
shows variable positivity for actin and desmin,
and is negative for other endothelial markers.
Imaging findings ( Fig. 3 ).
• Mammogram. When imaging findings are present,
circumscribed nodules or subtle focal asymmetry may be found.
• US.
Usually circumscribed hypoechoic nodules or no findings.
• MR.
An heterogeneous mass with T2 hyperintense spaces or non-mass enhancement usually with a progressive (type 1) curve.
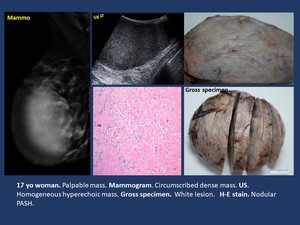
Fig. 3: Breast-specific stroma. Pseudoangiomatous stromal hyperplasia (PASH).
2.1.2.Phyllodes tumor.
It is a fibroepihelial lesion.
Phyllodes tumors are biphasic lesions,
with different types of specialized and non-specialized stroma in which the non-specialized stroma is the neoplastic component and determines its aggressiveness.
Benign and malignant phyllodes tumors are enlarging breast masses.
Recurrence may appear in all the cases.
On core biopsy differential diagnosis is difficult between phyllodes tumor and fibroadenoma.
When a mass diagnosed as fibroadenoma on core biopsy increases in size,
excluding phyllodes tumor is mandatory.
Imaging findings ( Fig. 4 ).
• Mammogram. Circumscribed mass.
• US.
Smooth margins and heterogeneous mass sometimes with cystic areas.
• MR.
Circumscribed mass,
with contrast enhancement.
In certain studies hyperintense T1 lesions are shown to be more frequently malignant.
Lesions which are iso and hypointense on T2 and with low ADC may correlate with stromal hypercellularity.
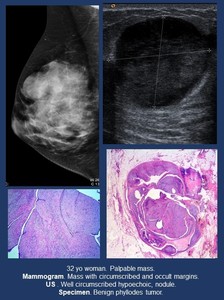
Fig. 4: Breast-specific stroma. Phyllodes tumor.
2.2. Non- specific stroma.
2.2.1.Fibrous tissue .
-Fibromatosis.
It is an infiltrative locally aggressive proliferation of fibroblasts/myofibroblasts. Presentation is usually a painless slow-growing ill-defined mass.
Gross pathologic features are sometimes a stellate lesion.
On immunohistochemistry it is negative for CD34,
CKs,
p63,
desmin,
and S100.
Imaging findings ( Fig. 5 ).
• Mammogram and US. Ill-defined or spiculated mass.
It may simulate carcinoma.
• MR. Masses,
Isointense on T1-weighted and lower or higher intensity lesions on T2,
usually with heterogeneous contrast enhancement atypical for carcinoma
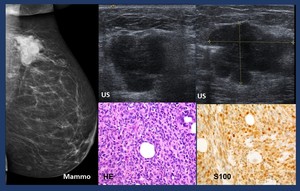
Fig. 22: Metastatic melanoma.- Mammogram. Dense mass with lobulated margins.
US.Heterogeneous mass with irregular margins.
HE. Melanoma.
- Nodular fasciitis.
Lesion composed of Fibroblasts.
Clinically they present as tender or painful rapidly growing breast mass.
On pathology mitosis may be frequent,
but no abnormal forms appear. On immunohistochemistry (IHC) it is positive for actin.
Imaging findings ( Fig. 6 ).
• Mammogram. Circumscribed or irregular masses sometimes mimicking malignancy.
• US. Irregular,
non-circumscribed hypoechoic nodules.
• MR. Irregular margins and contrast enhancement may appear,
usually with a type 1 curve.
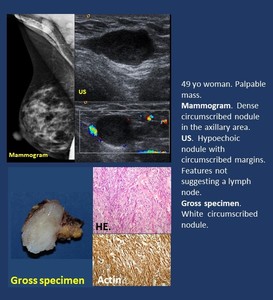
Fig. 6: Non-specific stroma. Fibrous tissue. Nodular fasciitis.
- Sarcoma.
Breast sarcomas are aggressive uncommon malignancies of the extrinsic connective tissue,
of different types.
Imaging findings ( Fig. 7 ).
• Mammogram. Usually big,
progressively growing non-specific mass,
usually with indistinct margins.
Osteogenic sarcoma shows specific osteoid matrix.
• US.
Heterogeneous mass,
usually hypoechoic and hypervascular,
sometimes with cystic areas.
• MR.
Heterogeneous,
usually big masses.
Irregular margins ,
usually T2 hyperintense an with inhomogeneous enhancement.
Differential diagnosis. Imaging features are not easily distinguished from ductal breast cancer,
but huge,
rapidly growing ,
heterogeneous and hypervascular suspicious masses may be sarcomas.

Fig. 7: Non-specific stroma. Fibrous tissue. Sarcoma.
2.2.2.Vascular lesions.
Pure vascular lesions are a complex spectrum which may be divided into different categories.
• Benign: cavernous and capillary haemangiomas.
• Atypical: atypical haemangiomas, papillary endothelial hyperplasia,
angiomatosis and angiolymphoid hyperplasia with eosinophilia (epithelioid haemangioma).
• Lesions with malignant potential: haemangiopericytomas and epithelioid haemangioendotheliomas.
• Malignant: angiosarcoma.
-Hemangioma ( Fig. 8 ).
The benign group of vascular lesions are masses composed of dilated vessels.
Imaging findings.
· Mammogram. Asymmetric dilatation of veins or circumscribed masses.
· US.
Anechoic,
usually lobulated mass.
Color and pulsed Doppler demonstrate its vascular nature.
· MR.
Dilated vessels
Differential diagnosis.
Hypodermal fat contains the major vasculature of the skin,
so vascular lesions may arise in the subdermal tissue.
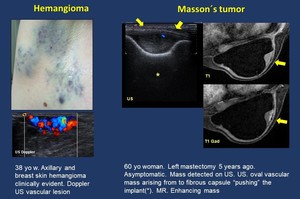
Fig. 8: Vascular lesions.
Hemangioma. Masson´s tumor.
-Atypical lesions.
Papillary endothelial hyperplasia of the breast.
Masson´s tumor ( Fig. 8 ).
It is a rare benign vascular lesion,
consisting of proliferating endothelial cells originating papillary structures.
It usually appears in the skin and soft tissues and may be found in different body locations.
Pathological analysis is required for diagnosis
Imaging findings.
• Mammogram,
US.
Circumscribed massses are found in all imaging modalities
• MR.
Usually heterogenously enhancing lesions on MR T1-weighted studies with gadolinium
-Angiosarcoma ( Fig. 9 ).
They may be primary within the breast parenchyma or secondary (parenchyma,
skin or chest wall) as a complication of radiation therapy.
Imaging findings.
Imaging findings are similar to sarcomas.
• Mammogram. Usually big,
progressively growing non-specific mass,
usually with indistinct margins.
Osteogenic sarcoma shows specific osteoid matrix.
• US.
Heterogeneous mass,
usually hypoechoic and hypervascular,
sometimes with cystic areas.
• MR.
Heterogeneous,
usually big masses.
Irregular margins ,
usually T2 hyperintense an with inhomogeneous enhancement.
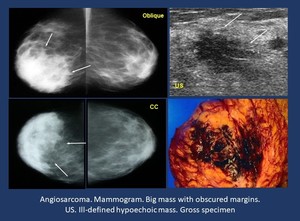
Fig. 9: Vascular lesions.
Angiosarcoma.
2.2.3.
Nerves .
Neurofibroma ( Fig. 10 ).
Patients with neurofibromatosis type I develop neurofibromas in the subcutaneous tissue which may also appear in the breast skin.
Imaging findings.
• Mammogram.
Small,
well-circumscribed nodules
• US.
Multiple hypoechoic masses within the subcutaneous fat tissue.
• MR.
Usually T1 hypointense,
T2 hyperintense with heterogeneous contrast enhancement.
Some of them have a typic target-like appearance.
Differential diagnosis.
Non-targetlike lesions may resemble lymphatic or venous malformation,
hemangioma or inflammatory subcutaneous lesions.
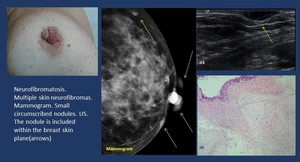
Fig. 10: Nervous tissue. Neurofibroma.
2.2.4.
Fatty tissue .
- Lipoma ( Fig. 11 ).
Palpable mass or asymptomatic lesion.
Imaging findings.
• Mammogram. Hypodense lesion,
sometimes not visible within normal fatty tissue.
• US. Circumscribed nodules with different appearances either hypoechoic,
heterogeneous or hyperechoic
• MR. circumscribed lesion with thin capsule and fatty tissue hyperintense T1,
hypointense T2.

Fig. 11: Fatty tissue. Lipoma
- Hamartoma ( Fig. 12 ).
It is a benign circumscribed and usually encapsulated mass,
with all the components of breast including different percentage of fatty tissue.
Imaging findings.
• Mammogram. A well-circumscribed heterogeneous mass containing densities similar to fat and soft tissue,
sometimes with a fine capsule,
but it may also be a homogeneous dense lesion.
• US. Heterogeneous or uniformly hypoechoic circumscribed masses.
• MR.
Depending on the amount of fat features vary.
Most frequently heterogenous,
with hypointense rim,
and predominantly hyperintense T1,
hypointense T2.
-Fat necrosis ( Fig. 12 ).
It appears as a result of trauma or surgery,
and may present with different appearances,
sometimes simulating breast cancer.
Imaging findings.
• Mammogram. Rim calcifications,
spiculated mass
• US. Shadowing,
mass with echogenic rim
• MR. T1WI High signal,
STIR.
Low signal ("black hole") with fat suppression,T1WI C+ FS thin rim of peripheral enhancement may persist up to 1.5 years
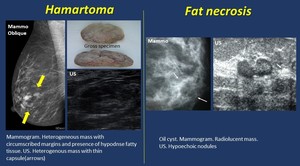
Fig. 12: Fatty tissue: Hamartoma. Fat necrosis.
2.2.5.
Lymphoid tissue .
-Lymphadenopathy.
Axillary and intramammary lymph nodes are common,
may be normal findings and are detected on imaging.
Pathologic lymph nodes in women´s breast or axilla should suggest invasive breast cancer in spite of the absence of breast lesions on mammography or US.
MR has greater sensitivity for detection of occult cancer.
Imaging findings.
• Mammogram. Circumscribed dense masses.
• US. Lymph nodes can be classified according to cortical morphologic features.
o Predominantly hyperechoic nodes are considered benign.
o Generalized cortical lobulation are usually benign, uncommonly a false-negative finding,
o The presence of asymmetric focal hypoechoic cortical lobulation or a completely hypoechoic node are suspicious for malignancy.
• MR. Circumscribed masses,
with fatty hilum,
lost in pathologic cases.
-Lymphoma ( Fig. 13 ,
Fig. 14 ,
Fig. 15 ).
Breast may hold primary (most B-cell) or secondary (secondary involvement of breast tissue by a systemic lymphoma/leukemia) lymphoma.
Imaging findings.
• Mammogram. Many different appearances may be found,
as well as multiple lymphadenopathy:
• A solitary,
round,
or oval mass with relatively circumscribed margins is the most common appearance.
• Spiculated or irregular margins may appear.
• Focal or diffuse increased density with or without skin thickening and sometimes breast enlargement may appear on mammography most frequently in high grade lesions.
• Less frequently architectural distortion or focal asymmetry.
• Normal mammogram may also appear.
• US.
Hypoechoic round masses with variable transmission sometimes ill-defined or hyperechoic.
Diffuse skin thickening may also appear.
• MR.
More commonly,
hyperintense masses on T2-weighted images and isointense on T1-weighted images.
Internal enhancement patterns are usually homogeneous with rapid initial and mixed delayed kinetics
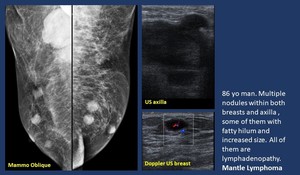
Fig. 13: Lymphadenopathy. Lymphoma.

Fig. 14: Lymphoma. Increased breast size.
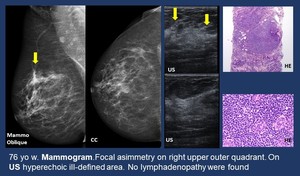
Fig. 15: MALT Lymphoma. Focal asymmetry.
2.2.6.
Muscle.
-Smooth muscle.
Leiomyomas.
Intraparenchymal leiomyomas of the breast are very rare smooth muscle benign tumors.
Leiomyoma of the nipple is a rare,
but more common,
benign neoplasm.
Presentation is usually a slowly growing mass.
Free margins should be established to prevent recurrence.
On IHC: positive for SMA,
desmin,
and caldesmon.
Imaging findings ( Fig. 16 ).
• Mammogram and US.
An oval mass with circumscribed margins.
• MR intermediate signal intensity on both T1- and T2-weighted images.
A dynamic MRI study shows enhancement.
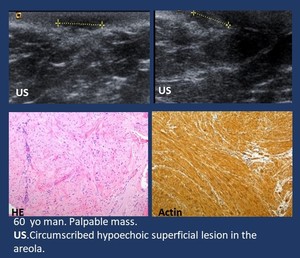
Fig. 16: Smooth muscle. Leiomyoma.
-Pectoralis muscle (skeletal muscle) ( Fig. 17 ).
Lesions arising in the pectoral major muscle may clinically simulate a breast mass.
Properly positioned mammogram,
US and MR depict the lesion,
being its location the main clue to diagnosis
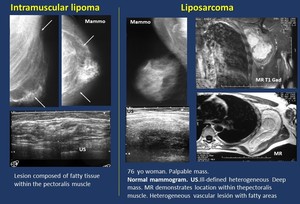
Fig. 17: Pectoralis muscle (Nearby structure).
Imaging findings.
· Mammogram. A radiolucent mass within the pectoralis muscle.
· US.
A deep,
well-cicumscribed heterogeneous mass beneath breast tissue.
· MR.
Features of fatty tissue lesion located within the pectoralis muscle.
- Malignant lesions.Liposarcoma.
Imaging findings.
· Mammogram.A mass within the pectoralis muscle or sometimes no findings due to its deep location in a patient with a palpable mass.
· US.
A deep heterogeneous mass.
· MR.Heterogeneous mass with different percentage of fatty tissue.
B.
Miscelanea.
Different lesions may be found infiltrating the breast,
and not properly arising from breast epithelium nor other components of the breast.
The main entities are:
1.Foreign bodies ( Fig. 18 ).
Foreign body granuloma may appear as an inflammatory reaction to certain substances.
Presence of different materials may be evident on mammograms and US sometimes with typical appearance.
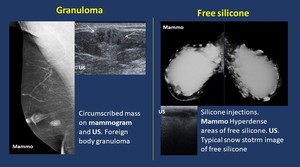
Fig. 18: Foreign bodies.
Free silicone.
Imaging findings.
· Mammogram. Dense opacities.
· US. Highly echogenic,
sometimes snowstorm appearance.
· MR. Low signal on fat suppressed T1,
high signal on water suppressed T2.
2.
Mastitis ( Fig. 19 ,
Fig. 20 ).
Inflammatory condition of the breast,
appearing most frequent during puerperal period.
Abscesses may appear as a complication of mastits.
Imaging findings.
· Mammogram. Signs of edema,
with thickened skin and increased breast density.
· US.Often hyperechoic areas.
· MR.
Thickened skin,
hyperintense areas on T2,
and sometimes contrast enhancement,
usually with a type 1 ascending curve.
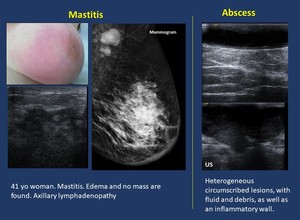
Fig. 19: Inflammatory. Mastitis
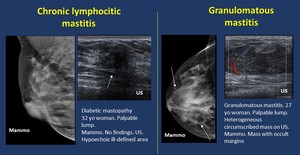
Fig. 20: Inflammatory. Mastitis
Differential diagnosis.
Inflammatory carcinoma.Inflammatory signs (edema or erythema) of skin (peau d´orange) of at least one-third of the breast.
· Pathology.
Dermal lymphatic vessels are involved,
obstructed or invaded by tumor emboli
· Imaging.
Edema and sometimes mass
· MR.
Patchy areas of mass-like and non-mass like enhancement
· When mass is present carcinoma should be excluded.
In all cases of mastitis follow up until complete resolution is mandatory.
- Chronic lymphocitic mastitis.
Unusual and probably immune-mediated.
If associated with diabetes it would be referred to as Diabetic mastopathy.
When the lymphocitic infiltrates associate lobular atrophy and sclerosis: Sclerosing type.
Inflammatory entity of unknown origin,
frequent in young women.
Clinically a mass,
sometimes ulcerated appears.
Imaging findings.
-
Mammogram. A mass or focal asymmetry may appear.
-
US.Often multiple tubular hypoechoic structures appear within the mass,
which is usually hypoechoic.
-
MR.A mass with contrast enhancement,
usually with ascending or plateau curve.
3.
Hematoma.
Hematoma appears usually after trauma.
History of previous trauma,
skin hematoma and regression within weeks are the keys to diagnosis.
Imaging findings ( Fig. 21 ).
-
Mammogram.
First an ill-defined lesion appears,
turning into a circumscribed lesion as it organizes. Calcification may appear sometimes in the long-term.
-
US.
Heterogeneous complex lesions varying from hyper to hypoechoic lesions during organization.
-
MR.Findings depend on the age of the hematoma
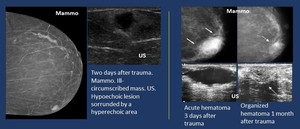
Fig. 21: Trauma. Hematoma.
4.
Metastases.
Different tumors can metastasize in breast parenchyma.,
being the most frequent melanoma
Clinical history and immunohistochemistry are keys for diagnosis.
Pathology.
Clues to diagnosis of metastases: unusual morphology,
lack of in situ component,
histology of primary.
Imaging findings ( Fig. 22 ).
-
Mammogram and US. Solitary or multiple masses.
Most common presentation solitary mass in the upper outer quadrant.
-
MR. Non-specific masses,
but some lesions such as melanoma may present specific features (Hyperintense on T1,
contrast enhancement).
Differential diagnosis. Presence of multiple masses may indicate metastasis,
but a solitary metastasis may also appear.
Fig. 22: Metastatic melanoma.- Mammogram. Dense mass with lobulated margins.
US.Heterogeneous mass with irregular margins.
HE. Melanoma.



.")













.")




