The inferior vein cava is the main conduit of venous return to the right atrium from the lower extremities and abdominal viscera.
It is formed by the confluence of the right and left common iliac veins,
which drain blood from the lower extremities and pelvis.
As it ascends in the retroperitoneum to the right of the abdominal aorta,
the IVC receives blood from the lumbar veins,
the left and right renal veins,
the right gonadal vein,
and the hepatic veins.
The azygos venous system connects to the IVC either directly or through the renal veins.
The IVC and its branches are best seen in the coronal plane.
Imaging techniques
Imaging anomalies of the IVC is sometimes challenging because most of them are unexpected (found in studies performed for staging malignancies,
for the study of non-specific abdominal symptoms or for other reasons).The radiological study of this vessel can be made by ultrasound,
computed tomography or MRI.
The last two are the most sensitive imaging techniques to depict congenital anomalies and pathology of this vessel.
However,
each of the three techniques has different advantages and disadvantages:
Color Doppler ultrasound
Ultrasound is available,
rapid and has no radiation.
However,
it is operator dependent,
and visualization of the IVC (especially the infrahepatic portion) may be difficult due to bowel gas or obesity (Fig.
1).
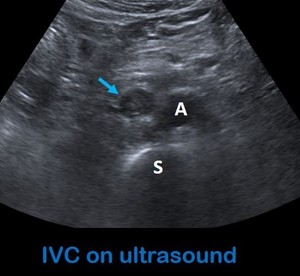
Fig. 1: Axial image of ultrasound at the level of the retroperitoneum shows echogenic material inside the infrarenal IVC in keeping with a thrombus in a patient with a non-semynomatous tumor. A: aorta. S: spine.
Computed tomography
As previously mentioned,
anomalies in the IVC are usually unexpected and found in abdominal studies performed for other reasons.
Usual abdominal CT sequences include venous phase,
obtained after a scanning delay of 60–70 seconds after injection.
Venous phase allows good evaluation of the suprarenal IVC due to venous return from the kidneys.
However,
evaluation of the infrarenal IVC is more challenging because of the admixture of less opacified blood from the lower extremities.
The ideal timing for the study of the entire IVC includes a delay of 70-90 seconds,
and should be performed if pathology of the IVC is suspected.
Magnetic Resonance Imaging (MRI)
MR imaging is the most reliable technique for depicting the presence and extent of tumor thrombus,
although due to its limited availability and cost,
it is usually not routinely used.
Three-dimensional breath-hold T1-weighted MR imaging performed after the intravenous administration of contrast material and balanced steady- state free precession are the most robust MR imaging sequences for imaging the IVC (Fig.2).
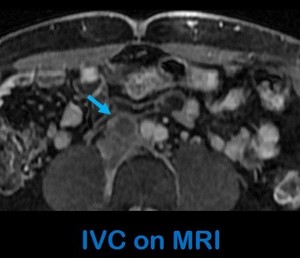
Fig. 2: Axial T1-W fat-supression contrast-enhanced MRI of the same patient shows occupation of the the infrarenal IVC (arrow) by enhancing material in keeping with a malignant thrombus.


 by enhancing material in keeping with a malignant thrombus.")