ECR 2018 / C-1774
Venous thrombosis and infection associated with peripherally inserted central catheter
Congress:
ECR 2018
Poster Number:
C-1774
Type:
Scientific Exhibit
Keywords:
Interventional vascular, Vascular, Extremities, Ultrasound-Colour Doppler, Ultrasound-Spectral Doppler, PACS, Catheters, Embolism / Thrombosis, Infection, Image verification
Authors:
A. Escobar, F. Puente, M. �. Carrillo, M. Del RÃo; Monterrey/MX
DOI:
10.1594/ecr2018/C-1774

Table 1

Fig. 2

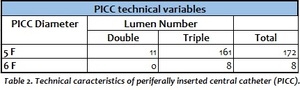
Table 2

Fig. 3

Fig. 4:
Gray scale duplex image in longitudinal view of left basilic vein shows the...

Fig. 5:
Gray scale duplex image in longitudinal view of left basilic vein shows the...

Fig. 6:
Gray scale duplex image in longitudinal view of left basilic vein shows the...

Fig. 7:
Gray scale ultrasound image shows the measurement of letf basilic vein in a...

Fig. 8:
Gray scale duplex image in longitudinal view of left basilic vein shows the...

Fig. 9:
Gray scale duplex image in longitudinal view of left basilic vein shows the...

Fig. 10:
Gray scale duplex image confirms the catheter position inside the left basilic...

Fig. 11:
A gray scale duplex image of left axilar vein shows an cute thrombus in a...

Fig. 12:
A gray scale duplex in a transverse view image shows no compression of the left...

Fig. 13:
Color Doppler ultrasonography of left axilar vein shows lack of venous flow.