We present our 15 years' experience with patients admitted to our Emergency Department with unclear acute scrotal pain.
Examinations consisted of high-resolution US,
CD at baseline,
low-mechanical index CEUS,
and contrast-enhanced power Doppler (PD).
Both testes were examined to compare their size,
echotexture,
and vascular features.
The examination was extended to the epididymal and funicular structures.
The acoustic contrast agent (Sonovue–Bracco,
Swiss) was administered as a rapid IV bolus (2.4-4.8 mL),
and the line was flushed with 5-10 mL of normal saline.
Images were acquired in real time for 3-6 min,
with occasional flashes to promote recirculation of the contrast medium.
Testicular torsion
It occurs when a testicle torts on the spermatic cord,
implying first venous and later arterial flow obstruction [6].
The extent of testicular ischemia will depend on the degree of twisting (180°–720°) and the duration of the torsion.
It can be “incomplete” or “complete” if the cord twists respectively <360° or >360°.
Baseline US findings are variables.
In the early phases of torsion (1–3 hours),
testicular echogenicity appears normal.
With progression,
enlargement of the affected testis and increased or heterogeneous echogenicity are common.
A definitive diagnosis of complete testicular torsion can be made when blood flow is visualized at CD/PD on the normal side,
resulting absent on the affected side.
Additional information can be obtained from pulsed-wave Doppler imaging,
which can demonstrate decreased or reversed diastolic flow on the affected side (Case 1).
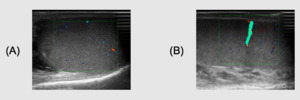
Fig. 1
References: Department of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
Fig. 2
References: Department of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)

Fig. 3
References: Department of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
Case 1.
Incomplete torsion in a 20-years-old patient admitted to Emergency Department with acute scrotal pain.
US with CD/PD demonstrates vascularity within the testis (Fig.1A),
although reducted comparing to the controlateral side (Fig.1B).
PD clearly depicts the torsion of the spermatic cord avoiding the use of CEUS.
(Fig.2-movie).
The diagnostic hypotesis was confirmed at surgery (Fig.3)
Diastolic flow and the flow curve may be difficult to demonstrate in infants,
small children and uncompliant patients [7].
In these selected cases,
CEUS can provide a quick diagnosis of acute testicular torsion,
showing the lack of enhancement of the affected side in the complete form.
This technique becomes problem solving in cases of incomplete torsion,
showing some residual vascularity of the affected testis (Case 2).
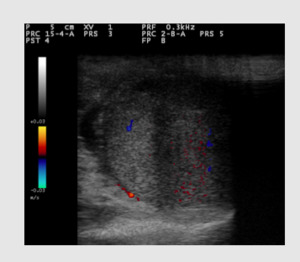
Fig. 4
References: Department of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
Fig. 5
References: Department of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
Case 2.
Incomplete torsion in a 18-years-old patient admitted to Emergency Department with acute scrotal pain.
US with CD demonstrates some sporadic vascular spots with diffuse artifacts,
due to movement of the patient and low PRF (Fig.4).
CEUS clearly shows the residual polar vascularization within the testis and normal enhancement of controlateral side (Fig.5-movie).
Acute inflammatory disease
Epididymo-orchitis is an extremely common clinical problem.
The clinical spectrum ranges from mild tenderness to a severe febrile illness with abscess formation.
Baseline US and CD are generally able to demonstrate the typical morphologic and hemodynamic changes of inflammatory conditions.
Baseline US generally shows multiple hypoechoic abnormalities within the testicular parenchyma,
with septal accentuation with foci of low reflectivity conforming to the lobular anatomy and an enlarged,
heterogeneous and hypoechoic (or hyperechoic in case of hemorrhage) epididymis.
Increased vascularity at CD/PD is the hallmark of scrotal infection,
representing hyperemia of both epididymis and testis [8].
CEUS could play a role in the investigation of their complications such as abscesses,
characterized by a strong rim enhancement and non-enhancing content (Case 3).
Testicular ischemia is a rare complication of epididymo-orchitis caused by extrinsic vascular compression.
CD and CEUS can quickly demonstrate the reduction or lack of vascularity of the affected side [9].
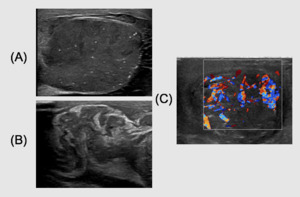
Fig. 6
References: Department of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
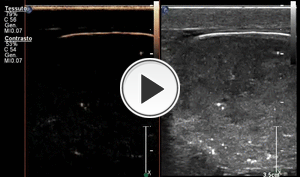
Fig. 7
References: Department of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
Case 3.
Complicated funicular-epidydimo-orchitis in a 45-years-old patient admitted to Emergency Department with acute scrotal pain and fever.
Baseline US demonstrates a swollen,
edematous and microlitiasic testis with inhomogenously hypoechoic band like areas,
especially in the upper pole (Fig.6A).
Enlarged and swollen funicolar cord at baseline US (Fig.6B).
PD shows increased vascularity within the testis (Fig.6C).
CEUS demostrates an apical area of necrosis and abscess-like perfusion of the band like areas,
with rim and paraseptal enhancement in the middle and lower pole of the testis (Fig.7-movie).
Trauma
Traumatic causes include blunt trauma (usually related to sports injuries and car accidents),
penetrating injuries and rare forms like electrical or thermal injuries.
Testicular trauma can produce contusions/hematomas,
hematoceles,
lacero-contusions/fractures,
and even testicular rupture [10].
Baseline US findings of testicular trauma are variable.
Up to one third of cases will show an echogenic fluid collection representing an acute hematocele.
Focal areas of altered parenchymal echogenicity may signify intratesticular hemorrhage or infarction,
not necessarily with evidence of testicular rupture.
CD can show the reduction of vascularity within contused parenchymal areas and allows to demonstrate the eventual residual vascularization within testicular fragments.
CEUS provides more complete information about testicular vascularization (essential for excluding infarctions) and about lesion features such as visibility,
size,
and margin characteristics,
sometimes not easy to evaluate at the baseline US.
Parenchymal lesions appear as markedly hypoperfused areas (focal contusions or laceration-contusions) or bands (fractures,
ruptures),
which are easy to distinguish from the background enhancement of the surrounding parenchyma [11].
In particular,
CEUS clearly can depict the fracture lines and the intratesticular and the extratesticular hematoma,
allowing sometimes to identify the interruption of the tunica albuginea,
hardly to distinguish at baseline US.
The detection of an interrupted tunica albuginea is crucial because a prompt surgery (within 72 h) can save the organ and preserve function (Case 4).
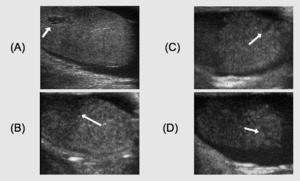
Fig. 8
References: Lobianco et al. Contrast-enhanced sonography in blunt scrotal trauma. Journal of Ultrasound. 2011;14(4):188-195.
Case 4.
Testicular rupture.
Baseline US reveals only a single testicular lesion (Fig.8A).
CEUS documents the presence of hypoperfusion caused by contusion injury to the upper mid—polar region,
not seen on baseline US (Fig.8B),
interruptions of the tunica albuginea (Fig.8C and D arrows),
and concomitant hematocele.
Neoplasm
Characterization of testicular painful mass is perhaps one of the most significant problem in the emergency setting.
Testicular tumors can present with an acute history of pain due to hemorrhage or infarction within the mass [12].
Although US has high sensitivity for detection of testicular processes,
its results may be inconclusive because of varied sonographic features not able to allow a definitive differential diagnosis.
CEUS may provide a more accurate assessment of the vascularity of testicular lesions than CD.
In particular the identification of wash in and wash out within a mass (Case 5) has a high positive predictive value of malignity (91-97,4 % as reported in literature).
On the contrary,
a benign lesion generally shows an early,
homogenous and persistent enhancement.
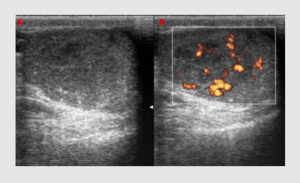
Fig. 9
References: Department of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)

Fig. 10
References: Department of Radiology, Santa Maria delle Grazie Hospital, Pozzuoli (Naples)
Case 5.
Seminoma in a 21-years-old patient admitted to Emergency Department with acute scrotal pain.
Baseline US reveals not well defined hypoechoic areas with periferal and central vascularization at PD (Fig.9).
CEUS demonstrates early enhancement and rapid wash-out of the lesion (Fig.10-movie),
allowing a diagnosis of malignant mass instead of an inflammatory disease,
then confirmed at biopsy.
