We wish to share the cross-sectional imaging features of various orbital pathologies that we encountered at our radiology department.
- A 16-slicer multidetector Toshiba CT scanner was used to perform the CT scans.
Additional 3D images and multiplanar reconstructions were acquired.
- MRI was performed on 1.5 Tesla Achieva Nova Philips scanner.
- Cases were followed till the histopathological results were obtained.
Orbital pathologies can be grossly devided into various etiologies:
- Trauma
- Infection / inflammation
- Vascular
- Neoplasia
TRAUMA:
INTRAOCULAR FOREIGN BODY: CT is the most sensitive and prompt technique for eveluation of orbital trauma and is usually the first imaging test performed.
Evaluation for non-metallic foreign bodies is more problematic,
and the CT was shown to be the most sensitive to demonstrate intraocular glass. Unlike metallic and glass material,
wooden foreign bodies usually appear hypoattenuating on CT.
In such cases,
MRI can demonstrate wooden foreign bodies.
Case # 1: A 32-year-old male patient came with recent history of road traffic accident.
He had swollwn right upper lid with chemosis. [Fig.
4]

Fig. 4: Intraocular metallic foreign body
LENS DISLOCATION: Blunt trauma to the eye can deform the globe which causes the zonular attachments that hold the lens in position to stretch and tear.
The lens may dislocate posteriorly or,
less commonly,
anteriorly. Nontraumatic lens dislocation can occur in systemic connective tissue disorders,
e.g.
Marfan syndrome,
Ehlers-Danlos syndrome and homocystinuria.
Case # 2: A 25-years-old male patient presenting after a motor vehicle accident with history of blunt trauma to the head.
Left eye was closed shut due to swelling and could not be clinically asessed. [Fig.
5]

Fig. 5: Traumatic posterior dislocation of lens with rupture of the globe along the right lateral aspect associated with preseptal edema and orbital engorgement.
ORBITAL HEMATOMA: Orbital hematoma is a common post-traumatic condition.
It can occur after facial and head trauma and involves rupture of orbital subperiosteal vessels.
In most cases patients present with proptosis,
diplopia and painful eyeball movement.
Case # 3: A 30-years-old male patient presented with history of blunt trauma one week earlier.
He had pain and swelling in left eye. [Fig.
6]
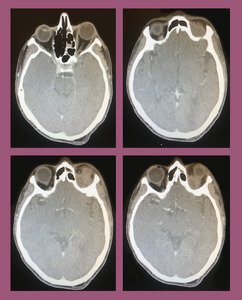
Fig. 6: Orbital Hematoma: Contrast enhanced axial CT scan shows a hyperdense mass in the retrobulbar region of left orbit associated with mild adjacent fat stranding. Imaging findings and patient's history were in keeping with retrobulbar orbital hematoma.
INFECTION / INFLAMMATION
DACROCYCTOCELE: These are caused by obstruction of both the proximal and distal ends of the nasolacrimal duct.
An imperforate Hasner membrane causes the distal blockage,
but the cause of proximal obstruction is less clearly understood. Dacryocystoceles may be unilateral or bilateral and have no sex predilection.
Case # 4: A 12-years-old male patient presented with progressive tense swelling at the medial canthus of right eye. There was history of trauma to the right eye 5 years back. [Fig.
7]
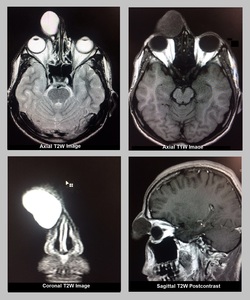
Fig. 7: Dacrocystocele: MRI Brain and Orbit was performed which showed a well-defined thin-walled abnormal signal intensity cystic mass arising from the lacrimal sac in medial canthus of right eye, producing a large bulge anteriorly. It was hypointense on T1W, hyperintense on T2W with no postcontrast enhancement or diffusion restriction. Findings represented dacrocystocele.
DACROCYSTITIS: It is the inflammation of the nasolacrrimal sac related to the impairment in the lacrimal drainage system and superimposed infection. This can be classified as congenital or acquired.
In adults the lacrimal sac or nasolacrimal duct can be obstructed by dacrolithiasis or debris which predisposes to infection. Dacryocystitis is typically characterised by epiphora,
erythema,
and oedema in the region of the medial epicanthus and lacrimal puncta as the result of an infection of the nasolacrimal sac. There is often mucopurulent discharge from the puncta and associated conjunctivitis.
Case # 5: A 50-years-old female patient presented with watery dischage from right eye since 15 days. [Fig.
8]

Fig. 8: Dacrocystitis: Plain CT shows an ill defined hyperdense fluid density medial epicanthal mass on the right side. It was centered over the the lacrimal sac. Associated pre-septal soft tissue standing was also noted. No post-septal inflammation was noted. No dacrolithiasis or subperiosteal abscess noted.
IDIOPATHIC ORBITAL MYOSITIS: It is a rare clinical condition characterized by idiopathic inflammation involving the extraocular muscles.
It most commonly affects patients in the third decade of life,
with a female predilection.
Patients typically present with acute eye or orbital pain,
decreased extra-ocular motility,
diplopia,
proptosis,
swollen eyelids,
and conjunctival hyperemia.
Visual acuity is typically spared.
The top differential are thyroid ophthalmopathy,
cellulitis,
Tolosa-Hunt syndrome,
and lymphoma.
Imaging include MRI of the orbits with and without contrast and with fat suppression.
CT of the orbits is a useful alternative if MRI is not readily available.
Case # 6: An 11 years old male patient presented with pain in his left eye.
The pain was worse with eye movement.
The patient denied any recent trauma,
history of autoimmune disease or thyroid abnormalities. [Fig.
9]

Fig. 9: Idiopathic Orbital Myositis: Non-enhanced CT imaging of the orbits showed marked enlargement of the left superior rectus muscle and tendon, with adjacent fat stranding. There was no apparent orbital abscess, thickening of the posterior sclera, or enlargement of the lacrimal gland. Patient was diagnosed as idiopathic orbital myositis and was started on oral prednisone. Three days later, his symptoms had fully resolved.
ORBITAL PSEUDOTUMOR: It is an idiopathic inflammatory condition that most commonly involves the extraocular muscles.
Less commonly there is inflammatory change involving the uvea,
sclera,
lacrimal gland and retrobulbar soft tissues.
Case # 7: A 32-years-old female patient came with complaint of left sided mild painful protosis since 1 week. There was no history of trauma or hyperthyroidism. [Fig.
10]
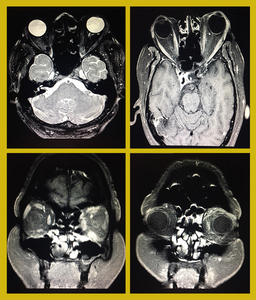
Fig. 10: Orbital Pseudotumor: Axial T2W FATSAT images show inhomogenous fat suppression in left-sided intraconal/ retrobulbar fat in the region of orbital apex with enhancement and stranding on post contrast T1W images. This represents orbital pseudotumor. There is thickening and enhancement of left inferior, medial and superior recti.
INVASIVE FUNGAL SINUSITIS: Is the most aggressive form of fungal sinusitis.
It is seen particularly in immunocompromised patients and is the source of significant morbidity and mortality. MRI is the modality of choice to assess soft tissue extension and intraorbital and intracranial extension.
Case # 8: A 40-years old diabetic patient presented with left chemosis and progressive proptosis since few weeks. [Fig.
11]
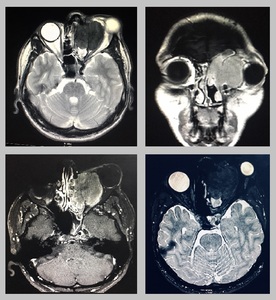
Fig. 11: Invasive fungal sinusitis: Contrast enhanced MRI shows a large abnormal signal intensity mass in the left ethmoid sinus causing destruction of the lamina papyracea with intraorbital extension on left side. It is also invading the left frontal sinus. It is causing mass effect on the globe and resulting in proptosis. It shows hyperintense signals on T1W sequence and intermediate signals on T2W images with marked contrast enhancement. Biopsy proven inavasive funal sinusitis.
THYROID OPHTHALMOPATHY: Thyroid ophthalmopathy or thyroid associated orbitopathy is the most common cause of proptosis in adults and is most frequently associated with Graves disease.
It is characterised by enlargement of the extra ocular muscles with increased orbital fat volume.
Case # 9: A 45-years-old hyperthyroid patient presented with progressive bilateral proptosis and reduced vision for 8 months. [Fig.
12]
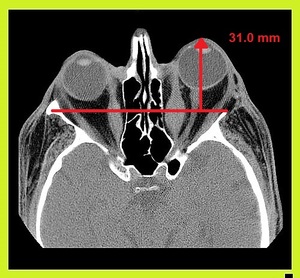
Fig. 12: Thyroid Ophthalmology: NECT shows bilateral symmetrical of the medial recti, predominantly involving the bellies with relative sparing of the tendons giving typical “coke bottle appearance”.
BENIGN PATHOLOGIES:
DERMOID / EPIDERMOID CYST: These are congenital lesions that develop as a result of sequestration of the ectoderm in the region of the orbit.
Focal thinning or scalloping of the adjacent bone may be seen in large deep dermoids.
Dermoid cysts may have cystic or solid components.
Case # 10: A 40-days-old female patient presented with proptosis of left eye since birth. [Fig.
13]
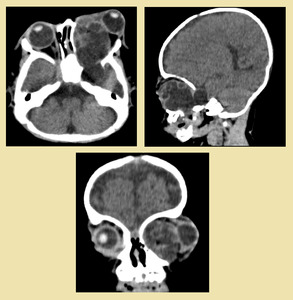
Fig. 13: Orbital epidermoid cyst: Non-enhanced CT revealed hypodense cystic mass (HU-110) in left temporal fossa extending into the ipsilateral orbital cavity, occupying the entire orbit, displacing its contents and causing pressure remodeling of the lamina papyracea. It was resulting in marked proptosis and widening of the orbital canal. Excisional biopsy proved epidermoid cyst.
Case # 11: A 16-years-old female patient presented with swelling her at left upper eye lid for 10 yrs. [Fig.
14]
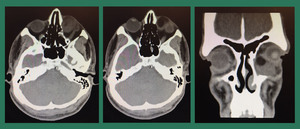
Fig. 14: Dermoid cyst: Plain CT showed an ovoid encapsulated mixed density area involving the inner and upper quadrant of the left orbit. There were fat density areas within the lesion showing Hounsfield units of -120. There was no evidence of underlying bony erosion or scalloping. Mass was closely abutting the globe which appeared unremarkable. No significant fat stranding was noted. No skin edema was noted. Findings were suggestive of dermoid cyst.
Case # 12: Another patient with swelling in the region of medial canthus of right eye since 6 years. [Fig.
15]
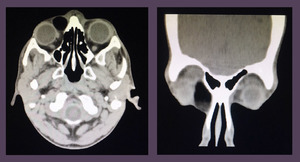
Fig. 15: Dermoid cyst: Plain CT showed a well circumscribed fat density lesion in the medial canthus of the right eye. Findings represented dermoid cyst. Patient underwent surgical excision of the lesion which was confirmed to be a dermoid cyst on histopathology.
FIBROUS DYSPLASIA:
Fibrous dysplasia is a developmental anomaly of bone in which fibro-osseous tissue replaces the normal bone marrow.
It represents about 5% of benign bone lesions. It can be monostotic or polyostotic.
Patients with subtle lesions are often asymptomatic,
otherwise can present with bone pain,
tenderness,
facial asymmetry,
vision problems and extraocular muscle palcies and swelling.
Ribs,
proximal femur,
humerus,
tibila and craniofacial bones are commonly involved in monostotic type or upto 75 % of skeleton can be involved in polyostotic type.
Case # 13: A 5-years-old female patient presented with facial asymmetry and bony prominence over the right temporal region.
Patient denied any pain,
double vision,
or tearing.
She denied any recent trauma. [Fig.
16]
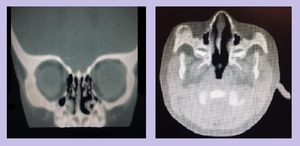
Fig. 16: Fibrous Dysplasia of greater wing of sphenoid bone: Nonenhanced CT scan showed expansion of the greater wing of the right sphenoid bone with ground glass appearance. There was no cortical break or associated soft tissue mass. The intraorbital contents appeared unremarkable. Findings suggested Craniofacial Fibrous Dysplasia.
VASCULAR PATHOLOGIES:
HEMANGIOMA: These are benign tumors of vascular origin lined by endothelial cells.
There are two recognized types involving the orbit i.e.
capillary haemangiomas and cavernous haemangiomas.
Capillary hemangiomas are one of the most common benign orbital tumors of infancy.
These presents after birth,
progressively increase in size then gradually involute.
These usually present with proptosis.
They can remodel or expand the bony orbit but erosion is not seen.
Imaging is used for the proper characterization and knowing the extent of the lesion. Cavernous haemangiomas are the most common benign orbital tumors in adults.
The typically present with painless proptosis,
lid swelling,
diplopia,
lump,
and recurrent obstructed vision.
They are mostly retrobulbar in location but can be found in extraconal location as well.
Case # 14: A 32 years old female patient presented with slowly progressing right sided proptosis,
diplopia and visual field defects. [Fig.
17]
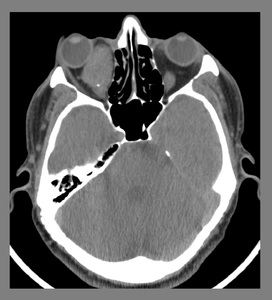
Fig. 17: Capillary hemangioma: An unenhanced CT scan showed a well circumscribed, ovoid soft tissue density mass with characteristic "speck of calcification" (phlebolith) occupying the right orbital cavity. It was causing marked displacement of the globe towards right side, compression over the optic nerve and expansion of the orbital cavity. Imaging findings represented orbital hemangioma.
Case # 15: A 13-years-old female patient presented with right sided proptosis and reduced vision. [Fig.
18]
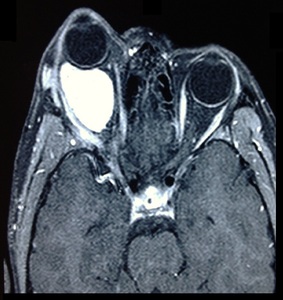
Fig. 18: Capillary Hemangioma: MRI of the brain with orbital protocol showed a large lobulated intraconal retro-orbital mass appearing heterogeneously low on T1W with intermediate signal intensity on T2W images. It showed intense post contrast enhancement. Anteriorly, it is pushing the globe causing proptosis. Anterolaterally, the mass was extending beyond the margins of the orbit causing periorbital edema. Laterally, it was expanding the orbital wall. Posteriorly, it was reaching up to the apex of orbit without intracranial extension. Medially, it was displacing & closely abutting the optic nerve which was seen throughout its course. Findings were suggestive of capillary hemangioma.
Case # 16: A 24-years-old female patient presented with left sided diplopia and proptosis.
There was also complaint of progressive swelling over her left cheek. [Fig.
19]
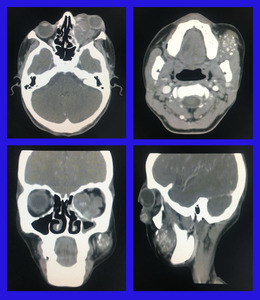
Fig. 19: Capillary hemangioma: A soft tissue density mass is seen in the extraconal compartment of left orbit causing marked left lateral displacement of the medial rectus and the globe. It is showing multiple specks of calcifications and post contrast enhancement. Another smaller lesion is seen in the intraconal compartment. Similar looking lesion was identified within the subcutaneous tissues of the left buccal mucosa.
MALIGNANT NEOPLASTIC:
RETINOBLASTOMA: These are the most common intraocular neoplasm found in childhood. Retinoblastomas may be sporadic or secondary to a germline mutation of the retinoblastoma suppressor gene),
which is usually inherited.
It may be unilateral or bilateral. Most cases are diagnosed within the first four years of life. Children with germline mutations are at increased risk of developing trilateral and quadrilateral varieties.
Trilateral retinoblastoma has bilateral retinoblastoma plus primitive neuroectodermal tumor arising in the pineal region or the suprasellar cistern.
Quadrilateral retinoblastoma present with bilateral ocular retinoblastom and tumors in both suprasellar and pineal regions.
Case # 17: A 3-years-old male child presented with reduced vision and white pupillary reflex in left eye since 4 months. [Fig. 20]
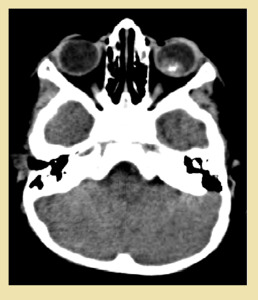
Fig. 20: Retinoblastoma: NECT scan showed a well-defined, soft tissue density intraocular retrolental mass on left side with few specks of calcification within it. The mass demonstrated heterogenous post contrast enhancement on contrast enhanced images. There was no evidence of intraconal or intracranial extension. Findings were suggestive of retinoblastoma. Histopathology confirmed the radiological findings.
Case # 16: An 18-months-old female child from a remote area presented with vision loss and large protruding mass from the left orbit.
One of the older sibling had similar complaint. [Fig.
21]
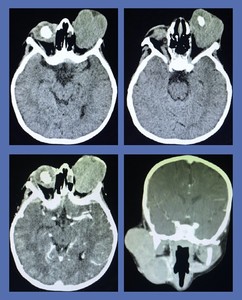
Fig. 21: Bilateral retinoblastoma: Contrast enhanced CT showed large bilateral enhancing intraocular masses. The mass on the left side was completely distorting the globe. It was associated with a large extraocular compoent extending outside the confines of the orbit resulting in marked proptosis. On unenhanced CT scan intraocular masses showed nodular clumps of calcification. Biopsy of the lesions confirmed bilateral retinoblastoma.
Case # 18: Another 2-years-old male child presented with bilateral white pupillary reflex in right eye and a large mass coming out of the left orbit. [Fig.
22]
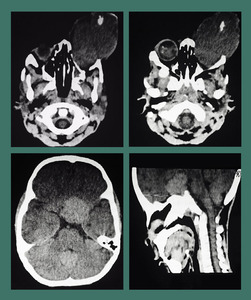
Fig. 22: Quadrilateral retinoblastoma: NECT scan showed bilateral intraocular masses containing nodular clumps of calcification. A large hyperdense masswas seen involving the suprasellar cistern suggesting neuroectodermal tumor. Imaging favoured bilateral retinoblastoma with primitive neuroectodermal tumor arising in the pineal region suggesting trilateral retinoblastoma.
Case # 19: A 12 months-old male child presented with bilateral white pupillary reflex since 1 month. [Fig.
23]
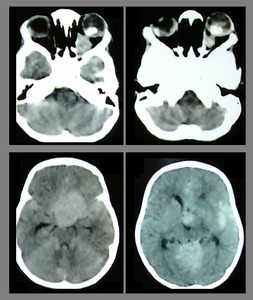
Fig. 23: Quadrilateral Retinoblastoma with cerebral metastasis: NECT scan showed bilateral well-defined soft tissue retrolental masses containing nodular clumps of calcification. There were huge hyperdense masses involving the suprasellar cistern and pineal region suggesting pineoblastoma and suprachiasmatic focus. Hyperdense areas were also seen in the cortical and subcortical regions suggesting parenchymal involvement indicative of cerebal metastasis. Imaging appearances favored quadrilateral retinoblastomas. According to the International Classification of Retinoblastoma imaging features represented Stage IV disease. Histopathology from the ocular lesion confirmed retinoblastoma.
RHABDOMYOSARCOMA:
Rhabdomyosarcoma is the most common primary orbital malignancy in children.
Most of the cases present below 6 years of age.
Invasion of the eyelid results in edema.
Pathologically Rhabdomyosarcoma develops from pluripotent mesenchymal cells that have the ability to differentiate into skeletal muscle.
Bone destruction and extension into anterior cranial fossa and paranasal sinuses can occur.
MRI and CT are needed for proper evaluation and knowing the extent of the mass.
Case # 20: A 4-years-old male child presented with rapidly developing proptosis and diplopia. [Fig.
24]
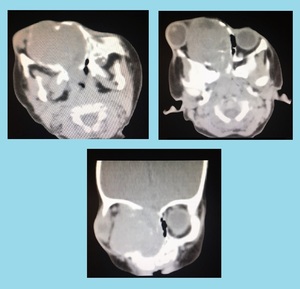
Fig. 24: Orbital Rhabdomyosarcoma: CECT showed a large soft tissue density mass is occupying the right orbital and nasal cavities. It is causing expansion of the orbit, marked proptosis of the globe, widening of the orbital canal and pressure remodeling of the adjacent bones. Findings were in favor of orbital rhabdomyosarcoma. Excisional biopsy confirmed the radiological diagnosis.
OPTIC NERVE MENINGIOMA: Optic nerve sheath meningiomas are the second most common optic nerve tumor following optic nerve glioma. The lesion derives from the arachnoid sheath of the optic nerve. Imaging features are characteristic,
such that biopsy is usually not warranted.
These may be associated with neurofibromatosis type 2.
Case # 21: A 38-years-old female patient came with complaint of slowly progressing painless proptosis and reduced visual acuity in left eye. [Fig.
25]
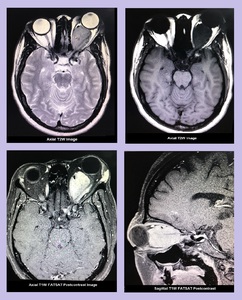
Fig. 25: Optic Nerve Meningioma: Contrast enhanced MRI Brain and Orbit showed a well-defined intraconal mass in left orbit, circumferentially encasing the left optic nerve. Anteriorly the mass was causing marked proptosis and posteriorly it was reaching up to the orbital apex and left cavernous sinus. It appeared hypointense on T1W and T2W images with avid post gadolinium enhancement. Findings represented optic nerve meningioma.
Case # 22: A 45-years-old female patient came with complaint of reduced visual acuity from right eye since 1 month. [Fig.
26]
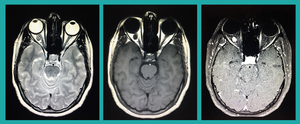
Fig. 26: Optic Meningioma: A small rounded saccular-shaped abnormal signal intensity mass is seen arising from the right optic nerve. It is appearing hypointense on T1W images and isointense on T2W images with intense enhancement on postcontrast T1W FATSAT images. No fat stranding or proptosis noted. Findings represent a mall optic nerve meningioma.
CHOROIDAL MELANOMA: Choroidal melanoma is the most common primary intraocular malignancy.
These tumours are identified incidentally on fundoscopy or as a result of retinal detachment or advanced disease. MRI is the modality of choice. Choroidal or ciliary body tumours are only identified incidentally on fundoscopy or as a result of retinal detachment or advanced disease.
Case # 23: A 35-years-old male patient presented with reduced visual acuity on right sided.
There was no history of trauma.
A mass was visualized on opthalmologic examination. [Fig.
27]
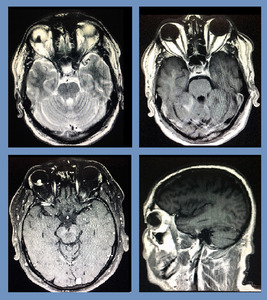
Fig. 27: Choroidal Melanoma: Contrast enhanced MRI showed an abnormal signal intensity mass in the posterior compartment of right eye. It was appearing hyperintense on T1 W and hypointense on T2W images. It showed intense enhancement on T1W FATSAT post gadolinium sequences. No extraocular extension was noted. Radiological findings were consistent with choroidal melanoma. Patient was operated subsequently, and histopathological diagnosis of choroidal melanoma was confirmed.
Case # 24 : A 62-years-old female patient presented with reduced visual acuity on left side.
There was no history of trauma. [Fig.
28]
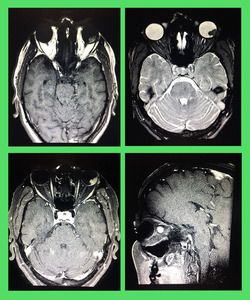
Fig. 28: Choroidal Melanoma: Contrast enhanced MRI showed an abnormal signal intensity mass in the posterior compartment of the left eye. It was appearing hyperintense on T1W and hypointense on T2W images. It showed intense enhancement on T1W FATSAT post gadolinium sequences. No extraocular extension was noted. Radiological findings were consistent with choroidal melanoma. Histopathology confirmed the radiological diagnosis.
CHONDROSARCOMA OF SPHENOID BONE: It is a malignant but usually slow-growing cartilaginous tumor.
It rarely occurs in the craniofacial region.
Because of its propensity to occur in the deep facial structures or base of the skull,
the true extent and origin of the tumor may be overlooked if not properly evaluated radiographically.
Case # 25: A 39-years-old female presented with progressive painless right sided proptosis for 2 years. [Fig.
29]
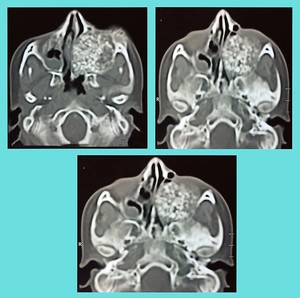
Fig. 29: Chondrosarcoma of sphenoid bone: CT scan demonstrates an extraaxial mixed density lesion shows chondroid matrix mineralization, arising from the greater wing of left sphenoid bone. It is causing bony erosion and destruction and is expanding into the orbital and nasal caivties causing their marked obliteration. Geometric center appeared to be at
junction of sphenoid and ethmoid sinuses. Biopsy proven chondrosarcoma.
ORBITAL METASTASIS: Orbital metastasis are relatively uncommon,
but some primary tumours do have a predilection to metastasise to the orbit.
These include melanoma,
breast and renal carcinoma.
Bone metastasis in advanced cases of buccal carcinoma is rarely reported in literature.
Case # 26: A 52-years-old male patient,
known case of buccal mucosal carcinoma presented with right sided proptosis. [Fig.
30]
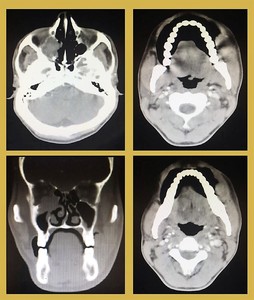
Fig. 30: Orbital metastasis: Contrast enhanced CT shows a destructive soft tissue extraconal lesion located at the apex of the right orbit causing destruction of the orbital floor. Paranasal sinuses appears unremarkable. Patient was a known case of left sided buccal mucosal carcinoma. Biopsy of the orbital lesion showed metastatic squamous cell carcinoma.










 in left temporal fossa extending into the ipsilateral orbital cavity, occupying the entire orbit, displacing its contents and causing pressure remodeling of the lamina papyracea. It was resulting in marked proptosis and widening of the orbital canal. Excisional biopsy proved epidermoid cyst.")



 occupying the right orbital cavity. It was causing marked displacement of the globe towards right side, compression over the optic nerve and expansion of the orbital cavity. Imaging findings represented orbital hemangioma.")












